- Future Students
- Current Students
- Faculty/Staff

News and Media
- News & Media Home
- Research Stories
- School’s In
- In the Media
You are here
More than two hours of homework may be counterproductive, research suggests.
")
A Stanford education researcher found that too much homework can negatively affect kids, especially their lives away from school, where family, friends and activities matter. "Our findings on the effects of homework challenge the traditional assumption that homework is inherently good," wrote Denise Pope , a senior lecturer at the Stanford Graduate School of Education and a co-author of a study published in the Journal of Experimental Education . The researchers used survey data to examine perceptions about homework, student well-being and behavioral engagement in a sample of 4,317 students from 10 high-performing high schools in upper-middle-class California communities. Along with the survey data, Pope and her colleagues used open-ended answers to explore the students' views on homework. Median household income exceeded $90,000 in these communities, and 93 percent of the students went on to college, either two-year or four-year. Students in these schools average about 3.1 hours of homework each night. "The findings address how current homework practices in privileged, high-performing schools sustain students' advantage in competitive climates yet hinder learning, full engagement and well-being," Pope wrote. Pope and her colleagues found that too much homework can diminish its effectiveness and even be counterproductive. They cite prior research indicating that homework benefits plateau at about two hours per night, and that 90 minutes to two and a half hours is optimal for high school. Their study found that too much homework is associated with: • Greater stress : 56 percent of the students considered homework a primary source of stress, according to the survey data. Forty-three percent viewed tests as a primary stressor, while 33 percent put the pressure to get good grades in that category. Less than 1 percent of the students said homework was not a stressor. • Reductions in health : In their open-ended answers, many students said their homework load led to sleep deprivation and other health problems. The researchers asked students whether they experienced health issues such as headaches, exhaustion, sleep deprivation, weight loss and stomach problems. • Less time for friends, family and extracurricular pursuits : Both the survey data and student responses indicate that spending too much time on homework meant that students were "not meeting their developmental needs or cultivating other critical life skills," according to the researchers. Students were more likely to drop activities, not see friends or family, and not pursue hobbies they enjoy. A balancing act The results offer empirical evidence that many students struggle to find balance between homework, extracurricular activities and social time, the researchers said. Many students felt forced or obligated to choose homework over developing other talents or skills. Also, there was no relationship between the time spent on homework and how much the student enjoyed it. The research quoted students as saying they often do homework they see as "pointless" or "mindless" in order to keep their grades up. "This kind of busy work, by its very nature, discourages learning and instead promotes doing homework simply to get points," said Pope, who is also a co-founder of Challenge Success , a nonprofit organization affiliated with the GSE that conducts research and works with schools and parents to improve students' educational experiences.. Pope said the research calls into question the value of assigning large amounts of homework in high-performing schools. Homework should not be simply assigned as a routine practice, she said. "Rather, any homework assigned should have a purpose and benefit, and it should be designed to cultivate learning and development," wrote Pope. High-performing paradox In places where students attend high-performing schools, too much homework can reduce their time to foster skills in the area of personal responsibility, the researchers concluded. "Young people are spending more time alone," they wrote, "which means less time for family and fewer opportunities to engage in their communities." Student perspectives The researchers say that while their open-ended or "self-reporting" methodology to gauge student concerns about homework may have limitations – some might regard it as an opportunity for "typical adolescent complaining" – it was important to learn firsthand what the students believe. The paper was co-authored by Mollie Galloway from Lewis and Clark College and Jerusha Conner from Villanova University.
Clifton B. Parker is a writer at the Stanford News Service .
More Stories

⟵ Go to all Research Stories
Get the Educator
Subscribe to our monthly newsletter.
Stanford Graduate School of Education
482 Galvez Mall Stanford, CA 94305-3096 Tel: (650) 723-2109
- Contact Admissions
- GSE Leadership
- Site Feedback
- Web Accessibility
- Career Resources
- Faculty Open Positions
- Explore Courses
- Academic Calendar
- Office of the Registrar
- Cubberley Library
- StanfordWho
- StanfordYou
Improving lives through learning
- Stanford Home
- Maps & Directions
- Search Stanford
- Emergency Info
- Terms of Use
- Non-Discrimination
- Accessibility
© Stanford University , Stanford , California 94305 .
Does Homework Really Help Students Learn?
A conversation with a Wheelock researcher, a BU student, and a fourth-grade teacher

“Quality homework is engaging and relevant to kids’ lives,” says Wheelock’s Janine Bempechat. “It gives them autonomy and engages them in the community and with their families. In some subjects, like math, worksheets can be very helpful. It has to do with the value of practicing over and over.” Photo by iStock/Glenn Cook Photography
Do your homework.
If only it were that simple.
Educators have debated the merits of homework since the late 19th century. In recent years, amid concerns of some parents and teachers that children are being stressed out by too much homework, things have only gotten more fraught.
“Homework is complicated,” says developmental psychologist Janine Bempechat, a Wheelock College of Education & Human Development clinical professor. The author of the essay “ The Case for (Quality) Homework—Why It Improves Learning and How Parents Can Help ” in the winter 2019 issue of Education Next , Bempechat has studied how the debate about homework is influencing teacher preparation, parent and student beliefs about learning, and school policies.
She worries especially about socioeconomically disadvantaged students from low-performing schools who, according to research by Bempechat and others, get little or no homework.
BU Today sat down with Bempechat and Erin Bruce (Wheelock’17,’18), a new fourth-grade teacher at a suburban Boston school, and future teacher freshman Emma Ardizzone (Wheelock) to talk about what quality homework looks like, how it can help children learn, and how schools can equip teachers to design it, evaluate it, and facilitate parents’ role in it.
BU Today: Parents and educators who are against homework in elementary school say there is no research definitively linking it to academic performance for kids in the early grades. You’ve said that they’re missing the point.
Bempechat : I think teachers assign homework in elementary school as a way to help kids develop skills they’ll need when they’re older—to begin to instill a sense of responsibility and to learn planning and organizational skills. That’s what I think is the greatest value of homework—in cultivating beliefs about learning and skills associated with academic success. If we greatly reduce or eliminate homework in elementary school, we deprive kids and parents of opportunities to instill these important learning habits and skills.
We do know that beginning in late middle school, and continuing through high school, there is a strong and positive correlation between homework completion and academic success.
That’s what I think is the greatest value of homework—in cultivating beliefs about learning and skills associated with academic success.
You talk about the importance of quality homework. What is that?
Quality homework is engaging and relevant to kids’ lives. It gives them autonomy and engages them in the community and with their families. In some subjects, like math, worksheets can be very helpful. It has to do with the value of practicing over and over.

What are your concerns about homework and low-income children?
The argument that some people make—that homework “punishes the poor” because lower-income parents may not be as well-equipped as affluent parents to help their children with homework—is very troubling to me. There are no parents who don’t care about their children’s learning. Parents don’t actually have to help with homework completion in order for kids to do well. They can help in other ways—by helping children organize a study space, providing snacks, being there as a support, helping children work in groups with siblings or friends.
Isn’t the discussion about getting rid of homework happening mostly in affluent communities?
Yes, and the stories we hear of kids being stressed out from too much homework—four or five hours of homework a night—are real. That’s problematic for physical and mental health and overall well-being. But the research shows that higher-income students get a lot more homework than lower-income kids.
Teachers may not have as high expectations for lower-income children. Schools should bear responsibility for providing supports for kids to be able to get their homework done—after-school clubs, community support, peer group support. It does kids a disservice when our expectations are lower for them.
The conversation around homework is to some extent a social class and social justice issue. If we eliminate homework for all children because affluent children have too much, we’re really doing a disservice to low-income children. They need the challenge, and every student can rise to the challenge with enough supports in place.
What did you learn by studying how education schools are preparing future teachers to handle homework?
My colleague, Margarita Jimenez-Silva, at the University of California, Davis, School of Education, and I interviewed faculty members at education schools, as well as supervising teachers, to find out how students are being prepared. And it seemed that they weren’t. There didn’t seem to be any readings on the research, or conversations on what high-quality homework is and how to design it.
Erin, what kind of training did you get in handling homework?
Bruce : I had phenomenal professors at Wheelock, but homework just didn’t come up. I did lots of student teaching. I’ve been in classrooms where the teachers didn’t assign any homework, and I’ve been in rooms where they assigned hours of homework a night. But I never even considered homework as something that was my decision. I just thought it was something I’d pull out of a book and it’d be done.
I started giving homework on the first night of school this year. My first assignment was to go home and draw a picture of the room where you do your homework. I want to know if it’s at a table and if there are chairs around it and if mom’s cooking dinner while you’re doing homework.
The second night I asked them to talk to a grown-up about how are you going to be able to get your homework done during the week. The kids really enjoyed it. There’s a running joke that I’m teaching life skills.
Friday nights, I read all my kids’ responses to me on their homework from the week and it’s wonderful. They pour their hearts out. It’s like we’re having a conversation on my couch Friday night.
It matters to know that the teacher cares about you and that what you think matters to the teacher. Homework is a vehicle to connect home and school…for parents to know teachers are welcoming to them and their families.
Bempechat : I can’t imagine that most new teachers would have the intuition Erin had in designing homework the way she did.
Ardizzone : Conversations with kids about homework, feeling you’re being listened to—that’s such a big part of wanting to do homework….I grew up in Westchester County. It was a pretty demanding school district. My junior year English teacher—I loved her—she would give us feedback, have meetings with all of us. She’d say, “If you have any questions, if you have anything you want to talk about, you can talk to me, here are my office hours.” It felt like she actually cared.
Bempechat : It matters to know that the teacher cares about you and that what you think matters to the teacher. Homework is a vehicle to connect home and school…for parents to know teachers are welcoming to them and their families.
Ardizzone : But can’t it lead to parents being overbearing and too involved in their children’s lives as students?
Bempechat : There’s good help and there’s bad help. The bad help is what you’re describing—when parents hover inappropriately, when they micromanage, when they see their children confused and struggling and tell them what to do.
Good help is when parents recognize there’s a struggle going on and instead ask informative questions: “Where do you think you went wrong?” They give hints, or pointers, rather than saying, “You missed this,” or “You didn’t read that.”
Bruce : I hope something comes of this. I hope BU or Wheelock can think of some way to make this a more pressing issue. As a first-year teacher, it was not something I even thought about on the first day of school—until a kid raised his hand and said, “Do we have homework?” It would have been wonderful if I’d had a plan from day one.
Explore Related Topics:
- Share this story
Senior Contributing Editor

Sara Rimer A journalist for more than three decades, Sara Rimer worked at the Miami Herald , Washington Post and, for 26 years, the New York Times , where she was the New England bureau chief, and a national reporter covering education, aging, immigration, and other social justice issues. Her stories on the death penalty’s inequities were nominated for a Pulitzer Prize and cited in the U.S. Supreme Court’s decision outlawing the execution of people with intellectual disabilities. Her journalism honors include Columbia University’s Meyer Berger award for in-depth human interest reporting. She holds a BA degree in American Studies from the University of Michigan. Profile
She can be reached at [email protected] .
Comments & Discussion
Boston University moderates comments to facilitate an informed, substantive, civil conversation. Abusive, profane, self-promotional, misleading, incoherent or off-topic comments will be rejected. Moderators are staffed during regular business hours (EST) and can only accept comments written in English. Statistics or facts must include a citation or a link to the citation.
There are 81 comments on Does Homework Really Help Students Learn?
Insightful! The values about homework in elementary schools are well aligned with my intuition as a parent.
when i finish my work i do my homework and i sometimes forget what to do because i did not get enough sleep
same omg it does not help me it is stressful and if I have it in more than one class I hate it.
Same I think my parent wants to help me but, she doesn’t care if I get bad grades so I just try my best and my grades are great.
I think that last question about Good help from parents is not know to all parents, we do as our parents did or how we best think it can be done, so maybe coaching parents or giving them resources on how to help with homework would be very beneficial for the parent on how to help and for the teacher to have consistency and improve homework results, and of course for the child. I do see how homework helps reaffirm the knowledge obtained in the classroom, I also have the ability to see progress and it is a time I share with my kids
The answer to the headline question is a no-brainer – a more pressing problem is why there is a difference in how students from different cultures succeed. Perfect example is the student population at BU – why is there a majority population of Asian students and only about 3% black students at BU? In fact at some universities there are law suits by Asians to stop discrimination and quotas against admitting Asian students because the real truth is that as a group they are demonstrating better qualifications for admittance, while at the same time there are quotas and reduced requirements for black students to boost their portion of the student population because as a group they do more poorly in meeting admissions standards – and it is not about the Benjamins. The real problem is that in our PC society no one has the gazuntas to explore this issue as it may reveal that all people are not created equal after all. Or is it just environmental cultural differences??????
I get you have a concern about the issue but that is not even what the point of this article is about. If you have an issue please take this to the site we have and only post your opinion about the actual topic
This is not at all what the article is talking about.
This literally has nothing to do with the article brought up. You should really take your opinions somewhere else before you speak about something that doesn’t make sense.
we have the same name
so they have the same name what of it?
lol you tell her
totally agree
What does that have to do with homework, that is not what the article talks about AT ALL.
Yes, I think homework plays an important role in the development of student life. Through homework, students have to face challenges on a daily basis and they try to solve them quickly.I am an intense online tutor at 24x7homeworkhelp and I give homework to my students at that level in which they handle it easily.
More than two-thirds of students said they used alcohol and drugs, primarily marijuana, to cope with stress.
You know what’s funny? I got this assignment to write an argument for homework about homework and this article was really helpful and understandable, and I also agree with this article’s point of view.
I also got the same task as you! I was looking for some good resources and I found this! I really found this article useful and easy to understand, just like you! ^^
i think that homework is the best thing that a child can have on the school because it help them with their thinking and memory.
I am a child myself and i think homework is a terrific pass time because i can’t play video games during the week. It also helps me set goals.
Homework is not harmful ,but it will if there is too much
I feel like, from a minors point of view that we shouldn’t get homework. Not only is the homework stressful, but it takes us away from relaxing and being social. For example, me and my friends was supposed to hang at the mall last week but we had to postpone it since we all had some sort of work to do. Our minds shouldn’t be focused on finishing an assignment that in realty, doesn’t matter. I completely understand that we should have homework. I have to write a paper on the unimportance of homework so thanks.
homework isn’t that bad
Are you a student? if not then i don’t really think you know how much and how severe todays homework really is
i am a student and i do not enjoy homework because i practice my sport 4 out of the five days we have school for 4 hours and that’s not even counting the commute time or the fact i still have to shower and eat dinner when i get home. its draining!
i totally agree with you. these people are such boomers
why just why
they do make a really good point, i think that there should be a limit though. hours and hours of homework can be really stressful, and the extra work isn’t making a difference to our learning, but i do believe homework should be optional and extra credit. that would make it for students to not have the leaning stress of a assignment and if you have a low grade you you can catch up.
Studies show that homework improves student achievement in terms of improved grades, test results, and the likelihood to attend college. Research published in the High School Journal indicates that students who spent between 31 and 90 minutes each day on homework “scored about 40 points higher on the SAT-Mathematics subtest than their peers, who reported spending no time on homework each day, on average.” On both standardized tests and grades, students in classes that were assigned homework outperformed 69% of students who didn’t have homework. A majority of studies on homework’s impact – 64% in one meta-study and 72% in another – showed that take home assignments were effective at improving academic achievement. Research by the Institute for the Study of Labor (IZA) concluded that increased homework led to better GPAs and higher probability of college attendance for high school boys. In fact, boys who attended college did more than three hours of additional homework per week in high school.
So how are your measuring student achievement? That’s the real question. The argument that doing homework is simply a tool for teaching responsibility isn’t enough for me. We can teach responsibility in a number of ways. Also the poor argument that parents don’t need to help with homework, and that students can do it on their own, is wishful thinking at best. It completely ignores neurodiverse students. Students in poverty aren’t magically going to find a space to do homework, a friend’s or siblings to help them do it, and snacks to eat. I feel like the author of this piece has never set foot in a classroom of students.
THIS. This article is pathetic coming from a university. So intellectually dishonest, refusing to address the havoc of capitalism and poverty plays on academic success in life. How can they in one sentence use poor kids in an argument and never once address that poor children have access to damn near 0 of the resources affluent kids have? Draw me a picture and let’s talk about feelings lmao what a joke is that gonna put food in their belly so they can have the calories to burn in order to use their brain to study? What about quiet their 7 other siblings that they share a single bedroom with for hours? Is it gonna force the single mom to magically be at home and at work at the same time to cook food while you study and be there to throw an encouraging word?
Also the “parents don’t need to be a parent and be able to guide their kid at all academically they just need to exist in the next room” is wild. Its one thing if a parent straight up is not equipped but to say kids can just figured it out is…. wow coming from an educator What’s next the teacher doesn’t need to teach cause the kid can just follow the packet and figure it out?
Well then get a tutor right? Oh wait you are poor only affluent kids can afford a tutor for their hours of homework a day were they on average have none of the worries a poor child does. Does this address that poor children are more likely to also suffer abuse and mental illness? Like mentioned what about kids that can’t learn or comprehend the forced standardized way? Just let em fail? These children regularly are not in “special education”(some of those are a joke in their own and full of neglect and abuse) programs cause most aren’t even acknowledged as having disabilities or disorders.
But yes all and all those pesky poor kids just aren’t being worked hard enough lol pretty sure poor children’s existence just in childhood is more work, stress, and responsibility alone than an affluent child’s entire life cycle. Love they never once talked about the quality of education in the classroom being so bad between the poor and affluent it can qualify as segregation, just basically blamed poor people for being lazy, good job capitalism for failing us once again!
why the hell?
you should feel bad for saying this, this article can be helpful for people who has to write a essay about it
This is more of a political rant than it is about homework
I know a teacher who has told his students their homework is to find something they are interested in, pursue it and then come share what they learn. The student responses are quite compelling. One girl taught herself German so she could talk to her grandfather. One boy did a research project on Nelson Mandela because the teacher had mentioned him in class. Another boy, a both on the autism spectrum, fixed his family’s computer. The list goes on. This is fourth grade. I think students are highly motivated to learn, when we step aside and encourage them.
The whole point of homework is to give the students a chance to use the material that they have been presented with in class. If they never have the opportunity to use that information, and discover that it is actually useful, it will be in one ear and out the other. As a science teacher, it is critical that the students are challenged to use the material they have been presented with, which gives them the opportunity to actually think about it rather than regurgitate “facts”. Well designed homework forces the student to think conceptually, as opposed to regurgitation, which is never a pretty sight
Wonderful discussion. and yes, homework helps in learning and building skills in students.
not true it just causes kids to stress
Homework can be both beneficial and unuseful, if you will. There are students who are gifted in all subjects in school and ones with disabilities. Why should the students who are gifted get the lucky break, whereas the people who have disabilities suffer? The people who were born with this “gift” go through school with ease whereas people with disabilities struggle with the work given to them. I speak from experience because I am one of those students: the ones with disabilities. Homework doesn’t benefit “us”, it only tears us down and put us in an abyss of confusion and stress and hopelessness because we can’t learn as fast as others. Or we can’t handle the amount of work given whereas the gifted students go through it with ease. It just brings us down and makes us feel lost; because no mater what, it feels like we are destined to fail. It feels like we weren’t “cut out” for success.
homework does help
here is the thing though, if a child is shoved in the face with a whole ton of homework that isn’t really even considered homework it is assignments, it’s not helpful. the teacher should make homework more of a fun learning experience rather than something that is dreaded
This article was wonderful, I am going to ask my teachers about extra, or at all giving homework.
I agree. Especially when you have homework before an exam. Which is distasteful as you’ll need that time to study. It doesn’t make any sense, nor does us doing homework really matters as It’s just facts thrown at us.
Homework is too severe and is just too much for students, schools need to decrease the amount of homework. When teachers assign homework they forget that the students have other classes that give them the same amount of homework each day. Students need to work on social skills and life skills.
I disagree.
Beyond achievement, proponents of homework argue that it can have many other beneficial effects. They claim it can help students develop good study habits so they are ready to grow as their cognitive capacities mature. It can help students recognize that learning can occur at home as well as at school. Homework can foster independent learning and responsible character traits. And it can give parents an opportunity to see what’s going on at school and let them express positive attitudes toward achievement.
Homework is helpful because homework helps us by teaching us how to learn a specific topic.
As a student myself, I can say that I have almost never gotten the full 9 hours of recommended sleep time, because of homework. (Now I’m writing an essay on it in the middle of the night D=)
I am a 10 year old kid doing a report about “Is homework good or bad” for homework before i was going to do homework is bad but the sources from this site changed my mind!
Homeowkr is god for stusenrs
I agree with hunter because homework can be so stressful especially with this whole covid thing no one has time for homework and every one just wants to get back to there normal lives it is especially stressful when you go on a 2 week vaca 3 weeks into the new school year and and then less then a week after you come back from the vaca you are out for over a month because of covid and you have no way to get the assignment done and turned in
As great as homework is said to be in the is article, I feel like the viewpoint of the students was left out. Every where I go on the internet researching about this topic it almost always has interviews from teachers, professors, and the like. However isn’t that a little biased? Of course teachers are going to be for homework, they’re not the ones that have to stay up past midnight completing the homework from not just one class, but all of them. I just feel like this site is one-sided and you should include what the students of today think of spending four hours every night completing 6-8 classes worth of work.
Are we talking about homework or practice? Those are two very different things and can result in different outcomes.
Homework is a graded assignment. I do not know of research showing the benefits of graded assignments going home.
Practice; however, can be extremely beneficial, especially if there is some sort of feedback (not a grade but feedback). That feedback can come from the teacher, another student or even an automated grading program.
As a former band director, I assigned daily practice. I never once thought it would be appropriate for me to require the students to turn in a recording of their practice for me to grade. Instead, I had in-class assignments/assessments that were graded and directly related to the practice assigned.
I would really like to read articles on “homework” that truly distinguish between the two.
oof i feel bad good luck!
thank you guys for the artical because I have to finish an assingment. yes i did cite it but just thanks
thx for the article guys.
Homework is good
I think homework is helpful AND harmful. Sometimes u can’t get sleep bc of homework but it helps u practice for school too so idk.
I agree with this Article. And does anyone know when this was published. I would like to know.
It was published FEb 19, 2019.
Studies have shown that homework improved student achievement in terms of improved grades, test results, and the likelihood to attend college.
i think homework can help kids but at the same time not help kids
This article is so out of touch with majority of homes it would be laughable if it wasn’t so incredibly sad.
There is no value to homework all it does is add stress to already stressed homes. Parents or adults magically having the time or energy to shepherd kids through homework is dome sort of 1950’s fantasy.
What lala land do these teachers live in?
Homework gives noting to the kid
Homework is Bad
homework is bad.
why do kids even have homework?
Comments are closed.
Latest from Bostonia
This sha alum handles fenway park’s celebrity artists, bu alum chompon boonnak runs mahaniyom, one of greater boston’s hottest thai restaurants, champion of indie films, china scholar merle goldman dies, cfa alum jonathan knight is head of games for the new york times, a commitment to early childhood education, reading list: alum bonnie hammer publishes 15 lies women are told at work —plus fiction, poetry, and short stories, one good deed: jason hurdich (cas’97) is uniting the deaf community, one cup at a time, is our democracy at risk americans think so. bu experts talk about why—and the way forward, space force general b. chance saltzman is a bu alum, feedback: readers weigh in on a bu superager, the passing of otto lerbinger, and alum’s book fat church, law alum steven m. wise, who fought for animal rights, dies, pups wearing custom-designed veterinary collars get star treatment in alum’s new coffee-table book, using glamour for good: alum’s nonprofit organization brings clothes and beauty products to those in need, gallery: shea justice (cfa’93), oscar-nominated actor hong chau (com’01) stars in new action-comedy the instigators, alum’s new book recounts the battle for inclusion in boy scouts, opening doors: ellice patterson (questrom’17), an alum’s new memoir recounts six decades of beatlemania, bu alum in paris keeping olympians’ minds sharp and healthy.
Science of mind

Why is homework good for your brain?
Did you know that homework has a profound impact on brain development? It’s not just about completing assignments; homework can actually improve brain function and enhance cognitive abilities.
Homework is designed to help students prepare for the future and develop skills that are essential for success in life. It offers several cognitive benefits, including the development of memory and critical thinking skills. By practicing and repeating new skills through homework, students can enhance their memory and retain knowledge for exams and future tests.
But that’s not all. Homework also helps students build suitable study habits, learn time management, realize personal responsibility, work independently, and improve their ability to use resources and conduct research.
Key Takeaways:
- Homework improves brain function and enhances cognitive abilities.
- By practicing and repeating new skills through homework, students can enhance their memory and retain knowledge.
- Homework helps students build suitable study habits, learn time management, and realize personal responsibility.
- Homework fosters independence and the ability to use resources effectively.
- Research shows that designing and assigning homework correctly can optimize its effectiveness as a learning tool.
The Cognitive Benefits of Homework
Homework is not just a task assigned by teachers to keep students occupied after school; it has far-reaching cognitive benefits and contributes to brain growth and development. Through various homework assignments, students have the opportunity to enhance critical thinking skills, memory retention, and problem-solving abilities.
One essential cognitive benefit of homework is its ability to challenge and develop critical thinking skills. By applying the concepts they’ve learned in class to real-life situations, students can deepen their understanding and improve their analytical thinking abilities. This practice fosters a deeper level of comprehension and encourages students to actively engage with the material.
Another cognitive benefit of homework is its positive impact on memory retention. Through practice and repetition of new skills and knowledge, students reinforce the neural connections in their brains, making the information more accessible and easier to recall. This improved memory retention helps students perform better on exams and enhances their overall academic performance.
Homework also plays a crucial role in developing problem-solving abilities. Assignments that require students to think critically and find innovative solutions to complex problems help cultivate their analytical and logical thinking skills. These problem-solving abilities are essential for success in various aspects of life, from academic pursuits to professional careers.
Overall, homework has a profound impact on cognitive development, providing students with opportunities to enhance critical thinking, memory retention, and problem-solving abilities. By engaging in regular homework assignments, students can nurture these essential cognitive skills and lay a solid foundation for their future academic and professional success.
Building Essential Skills Through Homework
Homework plays a vital role in building essential skills that are crucial for academic success and beyond. It provides students with the opportunity to develop effective study habits, learn time management, cultivate personal responsibility, and engage in independent work.
One of the key benefits of homework is the development of study habits. Through regular homework assignments, students learn how to plan their study sessions, set realistic goals, and effectively organize their time. By following consistent study routines, students can maximize their learning potential and improve their overall academic performance.
Time management is another vital skill that homework helps students develop. By juggling multiple assignments and deadlines, students learn to prioritize tasks, allocate their time effectively, and meet their academic obligations. These skills are essential not only for academic success but also for managing responsibilities in other areas of life.
Homework also fosters a sense of personal responsibility. Being accountable for completing assignments on time and to the best of their ability teaches students the importance of taking ownership of their education. It instills a work ethic that can significantly impact their future success, both inside and outside the classroom.
Furthermore, homework promotes independent work and critical thinking skills. Through assignments that require students to apply concepts learned in class, they develop their problem-solving abilities and deepen their understanding of the subject matter. This type of independent work encourages students to think creatively, analyze information critically, and develop their own perspectives.
By engaging in homework, students are actively building these essential skills that will benefit them throughout their education and beyond. The combination of effective study habits, time management, personal responsibility, and independent work fosters self-discipline, resilience, and a lifelong love of learning.

Testimonial:
“Homework has been instrumental in developing my study habits and time management skills. It has taught me the importance of setting goals and staying organized. Through homework, I’ve become more accountable and independent in my learning.” – Jane Smith, High School Student
Homework and Research Skills
When it comes to homework, research skills are essential for academic success. Homework assignments often require students to explore various resources, such as research papers, books, websites, and videos. By delving into these resources, students develop the ability to effectively use different information sources and enhance their understanding of the subject matter.
Research skills acquired through homework not only improve students’ academic performance but also prepare them to navigate the vast amount of information available in the digital age. By honing their research skills, students become adept at finding relevant and reliable information, analyzing different sources, and critically evaluating the credibility and validity of the information they come across.
Research skills acquired through homework contribute to academic success and prepare students for future challenges.
Through homework, students develop the persistence and resilience necessary to delve deep into a topic, locate relevant information, and synthesize their findings in a coherent manner. These skills are not only valuable during their academic journey but will also benefit them throughout their lives as they continue to learn and grow.
Moreover, conducting research for homework assignments instills a sense of curiosity and a thirst for knowledge in students. It encourages them to explore beyond the textbook and develop a broader perspective on the topics they are studying. They learn to ask questions, seek answers, and develop a lifelong love for learning.
Overall, homework assignments that require research skills play a vital role in shaping students’ intellectual growth, fostering critical thinking, and preparing them for the challenges they will face in their future academic and professional endeavors.

| Benefits of Homework and Research Skills |
|---|
| 1. Develops the ability to use various information sources effectively |
| 2. Enhances critical thinking and analytical skills |
| 3. Improves understanding and knowledge retention |
| 4. Encourages curiosity and a love for learning |
| 5. Prepares students for academic and professional challenges |
The Science of Homework Efficiency
When it comes to homework, there is a science behind ensuring its maximum effectiveness as a learning tool. Research has shown that the way homework is designed and assigned can have a significant impact on student performance. To optimize learning outcomes, homework should provide independent learning opportunities and present challenges that facilitate deliberate practice of essential content and skills.
One factor that can greatly affect the efficiency of homework is task switching. Constantly switching between homework and distractions like social media can significantly prolong the time spent on assignments. To overcome this, it is crucial to encourage students to delay gratification by using social media as a reward after completing their assignments. By eliminating distractions and focusing on the task at hand, students can deepen their learning and complete their homework more efficiently.
Adopting a scientific approach to tackling homework can lead to improved academic performance. By implementing strategies that optimize learning, such as organizing study sessions, setting goals, and utilizing resources effectively, students can enhance their understanding of the subject matter and improve their overall learning outcomes. By prioritizing uninterrupted focus and disciplined work, students can transform homework into a valuable learning experience that prepares them for success in their academic endeavors.
Source Links
- https://www.crispebooks.org/
- http://www.math.usf.edu/~mccolm/pedagogy/HWgood.html
- https://www.edutopia.org/blog/homework-sleep-and-student-brain-glenn-whitman

Similar Posts

Is there a recommended exercise duration for brain health?

What Mushrooms Are Good For Brain Health?

How can I rewire my brain to be positive?

Can stress mess with your brain?

Can stress and anxiety cause brain problems?

Yoga’s Mental Health & Brain Benefits Revealed
The New York Times
Well | how exercise can help us learn.

How Exercise Can Help Us Learn

Gretchen Reynolds on the science of fitness.
Over the past decade, in study after study in animals and people, exercise has been shown to improve the ability to learn and remember. But the specifics of that process have remained hazy. Is it better to exercise before you learn something new? What about during? And should the exercise be vigorous or gentle?
Two new studies helpfully tackle those questions, with each reaching the conclusion that the timing and intensity of even a single bout of exercise can definitely affect your ability to remember — though not always beneficially.
To reach that conclusion, scientists conducting the larger and more ambitious of the new studies, published in May in PLoS One, first recruited 81 healthy young women who were native German speakers and randomly divided them into three groups. Each group wore headphones and listened for 30 minutes to lists of paired words, one a common German noun and the other its Polish equivalent. The women were asked to memorize the unfamiliar word.
But they heard the words under quite different circumstances. One group listened after sitting quietly for 30 minutes. A second group rode a stationary bicycle at a gentle pace for 30 minutes and then sat down and donned the headphones. And the third group rode a bicycle at a mild intensity for 30 minutes while wearing the headphones and listening to the new words.
Two days later, the women completed tests of their new vocabulary. Everyone could recall some new words. But the women who had gently ridden a bicycle while hearing the new words — who had exercised lightly during the process of creating new memories —performed best. They had the most robust recall of the new information, significantly better than the group that had sat quietly and better than the group that had exercised before learning. Those women performed only slightly better than the women who had not exercised at all.
That result contrasts tellingly with the findings of another new study of memory formation and exercise, presented in May at the annual meeting of the American College of Sports Medicine in Indianapolis. During this study, 11 female collegians read a dense chapter from a college textbook on two occasions: once while sitting quietly and, on a separate day, while exercising vigorously on an elliptical machine for 30 minutes. Immediately after each session, the students were tested on the material they’d just read. They were then retested the next day.
In this study, exercise did not help the women’s memories, at least in the short term. Their test scores were actually worse on the memory test conducted immediately after they’d exercised while reading compared with their scores taken soon after they’d been sitting quietly and studying.
But the recall gap disappeared the next day, when the women were retested. At that point, there were no differences in their scores, whether they’d vigorously exercised while learning the new material or not.
The message of these studies would seem to be that exercise timing and intensity interact to affect memory formation, said Maren Schmidt-Kassow, a professor at the Institute of Medical Psychology at Goethe University in Frankfurt, Germany, who led the study of gentle bicycling and memory. Exercising during learning was, in her study, significantly more effective than exercising beforehand or not exercising at all.
But that beneficial impact probably depended on the mildness of the workout, she said. Light-intensity exercise will elicit low but noticeable levels of physiological arousal, she said, which, in turn, presumably help to prime the brain for the intake of new information and the encoding of that information into memories.
If the exercise is more vigorous, however, it may overstimulate the body and brain, she said, monopolizing more of the brain’s attentional resources and leaving fewer for the creation of robust memories.
This theory also helps to explain why, in both studies, memory recall was best a day or two after exercise, by which time, Dr. Schmidt-Kassow said, physiological arousal would have dissipated.
Of course, the mysteries of human memory remain, by and large, mysteries. These new studies don’t explain how, for instance, at a molecular level, exercise affects the creation of individual memories. It is likely that, as part of the arousal process, exercise stimulates the release of certain chemicals in the brain that affect memory formation, Dr. Schmidt-Kassow said. But that idea has yet to be proven, although she and many other scientists have applicable studies underway.
For now, though, there is some practical takeaway from the current studies, said Walter Bixby, an associate professor at Elon University in North Carolina, who oversaw the study of vigorous exercise and reading. “If you have an exam” or other activity that involves memorizing and recalling information “in a few hours, you would probably be better off sitting quietly and studying,” he says. “However, if the exam is the next day, it won’t hurt you to study while exercising.” And if your workout is gentle, it could even help.
What's Next
Home > Blog > Tips for Online Students > The Pros and Cons of Homework
School Life Balance , Tips for Online Students
The Pros and Cons of Homework
Updated: July 16, 2024
Published: January 23, 2020

Remember those nights when you’d find yourself staring at a mountain of homework, eyes drooping, wondering if you’d ever see the light at the end of the tunnel? The debate over homework’s role in education is as old as time. Is it a crucial tool for reinforcing learning or just an unnecessary burden?
For college students, this question takes on new dimensions. Juggling homework with the endless amount of classes, part-time jobs, and social lives can feel like walking on thin ice. The pressure to maintain grades, meet deadlines, and still find time for friends and relaxation can be overwhelming. So, is homework a friend or foe?

Photo by energepic.com from Pexels
The homework dilemma.
A large amount of college students report feeling overwhelmed by their academic workload, leading to high levels of stress and anxiety. According to Research.com , 45% of college students in the U.S. experience “more than average” stress, with 36.5% citing stress as a major impediment to their academic performance. This stress often stems directly from the homework load, leading to symptoms like headaches, exhaustion, and difficulty sleeping. The intense pressure to manage homework alongside other responsibilities makes us question the true impact of homework on students’ overall well-being.
And then there’s the digital twist. A whopping 89% of students confessed to using AI tools like ChatGPT for their assignments. While these tools can be a godsend for quick answers and assistance, they can also undermine the personal effort and critical thinking necessary to truly understand the material.
On the brighter side, homework can be a powerful ally. According to Inside Higher Ed , structured assignments can actually help reduce stress by providing a clear learning roadmap and keeping students engaged with the material. But where’s the balance between helpful and harmful?
With these perspectives in mind, let’s dive into the pros and cons of homework for college students. By understanding both sides, we can find a middle ground that maximizes learning while keeping stress at bay.
The Pros of Homework
When thoughtfully assigned, homework can be a valuable tool in a student’s educational journey . Let’s explore how homework can be a beneficial companion to your studies:
Enhances Critical Thinking
Homework isn’t just busywork; it’s an opportunity to stretch your mental muscles. Those late-night problem sets and essays can actually encourage deeper understanding and application of concepts. Think of homework as a mental gym; each assignment is a new exercise, pushing you to analyze, synthesize, and evaluate information in ways that strengthen your critical thinking skills .
Time Management Skills
Do you ever juggle multiple deadlines and wonder how to keep it all together? Regular homework assignments can be a crash course in time management . They teach you to prioritize tasks, manage your schedule, and balance academic responsibilities with personal commitments. The ability to juggle various tasks is a skill that will serve you well beyond your college years.
Reinforcement of Learning
There’s a reason why practice makes perfect. Homework reinforces what you’ve learned in class, helping to cement concepts and theories in your mind. Understanding a concept during a lecture is one thing, but applying it through homework can deepen your comprehension and retention.
Preparation for Exams
Think of homework as a sound check and warm-up for exams. Regular assignments keep you engaged with the material, making it easier to review and prepare when exam time rolls around. By consistently working through problems and writing essays, you build a solid foundation that can make the difference between cramming and confident exam performance.
Encourages Independent Learning
Homework promotes a sense of responsibility and independence. It pushes you to tackle assignments on your own, encouraging problem-solving and self-discipline. This independence prepares you for the academic challenges ahead and the autonomy required in your professional and personal life.

The Cons of Homework
Despite its potential benefits, homework can also have significant downsides. Let’s examine the challenges and drawbacks of homework:
Impact on Mental Health
Homework can be a double-edged sword when it comes to mental health . While it’s meant to reinforce learning, the sheer volume of assignments can lead to stress and anxiety. The constant pressure to meet deadlines and the fear of falling behind can create a relentless cycle of stress. Many students become overwhelmed, leading to burnout and negatively impacting their overall well-being.
Limited Time for Other Activities
College isn’t just about hitting the books. It’s also a time for personal growth, exploring new interests, and building social connections. Excessive homework can eat into the time you might otherwise spend on extracurricular activities, hobbies, or simply hanging out with friends. This lack of balance can lead to a less fulfilling college experience. Shouldn’t education be about more than just academics?
Quality Over Quantity
When it comes to homework, more isn’t always better. Piling on assignments can lead to diminished returns on learning. Instead of diving deep into a subject and gaining a thorough understanding, students might rush through tasks just to get them done. This focus on quantity over quality can undermine the educational value of homework.
Inequity in Education
Homework can sometimes exacerbate educational inequalities. Not all students can access the same resources and support systems at home. While some might have a quiet space and access to the internet, others might struggle with distractions and lack of resources. This disparity can put certain students at a disadvantage, making homework more of a burden than a learning tool.
Dependence on AI Tools
With the advent of AI tools like ChatGPT , homework has taken on a new dimension. While these tools can provide quick answers and assistance, they also pose the risk of students becoming overly reliant on technology. This dependence can take away from the actual learning process, as students might bypass the critical thinking and effort needed to truly understand the material. Is convenience worth the potential loss in learning?
Finding the Balance
Finding the right balance with homework means tackling assignments that challenge and support you. Instead of drowning in a sea of tasks, focus on quality over quantity. Choose projects that spark your critical thinking and connect to real-world situations. Flexibility is key here. Recognize that your circumstances are unique, and adjusting your approach can help reduce stress and create a more inclusive learning environment. Constructive feedback makes homework more than just a chore; it turns it into a tool for growth and improvement.
It’s also about living a well-rounded college life. Don’t let homework overshadow other important parts of your life, like extracurricular activities or personal downtime. Emphasize independent learning and use technology wisely to prepare for future challenges. By balancing thoughtful assignments with your personal needs, homework can shift from being a burden to becoming a helpful companion on your educational journey, enriching your academic and personal growth.
Homework has its pros and cons, especially for college students. It can enhance critical thinking, time management, and learning, but it also brings stress, impacts mental health, and can become overwhelming. Finding the right balance is key.
Focus on quality assignments, maintain flexibility, and make sure your homework complements rather than dominates your life. With a thoughtful approach, homework can support your educational journey, fostering both academic success and personal growth.
How can I manage my time effectively to balance homework and other activities?
Create a schedule that allocates specific times for homework, classes, and personal activities. Use planners or digital calendars to keep track of deadlines and prioritize tasks. Don’t forget to include breaks to avoid burnout.
How can I reduce the stress associated with homework?
To manage stress, practice mindfulness techniques like meditation or deep breathing exercises. Break assignments into smaller, manageable tasks and tackle them one at a time. If needed, seek support from classmates, tutors, or mental health professionals.
Is using AI tools for homework cheating?
While AI tools like ChatGPT can be helpful for quick assistance, relying on them too much can hinder your learning process. Use them as a supplement rather than a replacement for your own effort and critical thinking.
How can teachers make homework more equitable?
Teachers can offer flexible deadlines, provide resources for students who lack them, and design assignments that account for different learning styles and home environments. Open communication between students and teachers can also help address individual challenges.
What are some strategies to make homework more meaningful?
Focus on quality over quantity by designing assignments that encourage deep thinking and application of knowledge. Integrate real-world problems to make homework more relevant and engaging. Provide constructive feedback to help students learn and grow from their assignments.
In this article
At UoPeople, our blog writers are thinkers, researchers, and experts dedicated to curating articles relevant to our mission: making higher education accessible to everyone. Read More
Homework – Top 3 Pros and Cons
Pro/Con Arguments | Discussion Questions | Take Action | Sources | More Debates

From dioramas to book reports, from algebraic word problems to research projects, whether students should be given homework, as well as the type and amount of homework, has been debated for over a century. [ 1 ]
While we are unsure who invented homework, we do know that the word “homework” dates back to ancient Rome. Pliny the Younger asked his followers to practice their speeches at home. Memorization exercises as homework continued through the Middle Ages and Enlightenment by monks and other scholars. [ 45 ]
In the 19th century, German students of the Volksschulen or “People’s Schools” were given assignments to complete outside of the school day. This concept of homework quickly spread across Europe and was brought to the United States by Horace Mann , who encountered the idea in Prussia. [ 45 ]
In the early 1900s, progressive education theorists, championed by the magazine Ladies’ Home Journal , decried homework’s negative impact on children’s physical and mental health, leading California to ban homework for students under 15 from 1901 until 1917. In the 1930s, homework was portrayed as child labor, which was newly illegal, but the prevailing argument was that kids needed time to do household chores. [ 1 ] [ 2 ] [ 45 ] [ 46 ]
Public opinion swayed again in favor of homework in the 1950s due to concerns about keeping up with the Soviet Union’s technological advances during the Cold War . And, in 1986, the US government included homework as an educational quality boosting tool. [ 3 ] [ 45 ]
A 2014 study found kindergarteners to fifth graders averaged 2.9 hours of homework per week, sixth to eighth graders 3.2 hours per teacher, and ninth to twelfth graders 3.5 hours per teacher. A 2014-2019 study found that teens spent about an hour a day on homework. [ 4 ] [ 44 ]
Beginning in 2020, the COVID-19 pandemic complicated the very idea of homework as students were schooling remotely and many were doing all school work from home. Washington Post journalist Valerie Strauss asked, “Does homework work when kids are learning all day at home?” While students were mostly back in school buildings in fall 2021, the question remains of how effective homework is as an educational tool. [ 47 ]
Is Homework Beneficial?
Pro 1 Homework improves student achievement. Studies have shown that homework improved student achievement in terms of improved grades, test results, and the likelihood to attend college. Research published in the High School Journal indicated that students who spent between 31 and 90 minutes each day on homework “scored about 40 points higher on the SAT-Mathematics subtest than their peers, who reported spending no time on homework each day, on average.” [ 6 ] Students in classes that were assigned homework outperformed 69% of students who didn’t have homework on both standardized tests and grades. A majority of studies on homework’s impact – 64% in one meta-study and 72% in another – showed that take-home assignments were effective at improving academic achievement. [ 7 ] [ 8 ] Research by the Institute for the Study of Labor (IZA) concluded that increased homework led to better GPAs and higher probability of college attendance for high school boys. In fact, boys who attended college did more than three hours of additional homework per week in high school. [ 10 ] Read More
Pro 2 Homework helps to reinforce classroom learning, while developing good study habits and life skills. Students typically retain only 50% of the information teachers provide in class, and they need to apply that information in order to truly learn it. Abby Freireich and Brian Platzer, co-founders of Teachers Who Tutor NYC, explained, “at-home assignments help students learn the material taught in class. Students require independent practice to internalize new concepts… [And] these assignments can provide valuable data for teachers about how well students understand the curriculum.” [ 11 ] [ 49 ] Elementary school students who were taught “strategies to organize and complete homework,” such as prioritizing homework activities, collecting study materials, note-taking, and following directions, showed increased grades and more positive comments on report cards. [ 17 ] Research by the City University of New York noted that “students who engage in self-regulatory processes while completing homework,” such as goal-setting, time management, and remaining focused, “are generally more motivated and are higher achievers than those who do not use these processes.” [ 18 ] Homework also helps students develop key skills that they’ll use throughout their lives: accountability, autonomy, discipline, time management, self-direction, critical thinking, and independent problem-solving. Freireich and Platzer noted that “homework helps students acquire the skills needed to plan, organize, and complete their work.” [ 12 ] [ 13 ] [ 14 ] [ 15 ] [ 49 ] Read More
Pro 3 Homework allows parents to be involved with children’s learning. Thanks to take-home assignments, parents are able to track what their children are learning at school as well as their academic strengths and weaknesses. [ 12 ] Data from a nationwide sample of elementary school students show that parental involvement in homework can improve class performance, especially among economically disadvantaged African-American and Hispanic students. [ 20 ] Research from Johns Hopkins University found that an interactive homework process known as TIPS (Teachers Involve Parents in Schoolwork) improves student achievement: “Students in the TIPS group earned significantly higher report card grades after 18 weeks (1 TIPS assignment per week) than did non-TIPS students.” [ 21 ] Homework can also help clue parents in to the existence of any learning disabilities their children may have, allowing them to get help and adjust learning strategies as needed. Duke University Professor Harris Cooper noted, “Two parents once told me they refused to believe their child had a learning disability until homework revealed it to them.” [ 12 ] Read More
Con 1 Too much homework can be harmful. A poll of California high school students found that 59% thought they had too much homework. 82% of respondents said that they were “often or always stressed by schoolwork.” High-achieving high school students said too much homework leads to sleep deprivation and other health problems such as headaches, exhaustion, weight loss, and stomach problems. [ 24 ] [ 28 ] [ 29 ] Alfie Kohn, an education and parenting expert, said, “Kids should have a chance to just be kids… it’s absurd to insist that children must be engaged in constructive activities right up until their heads hit the pillow.” [ 27 ] Emmy Kang, a mental health counselor, explained, “More than half of students say that homework is their primary source of stress, and we know what stress can do on our bodies.” [ 48 ] Excessive homework can also lead to cheating: 90% of middle school students and 67% of high school students admit to copying someone else’s homework, and 43% of college students engaged in “unauthorized collaboration” on out-of-class assignments. Even parents take shortcuts on homework: 43% of those surveyed admitted to having completed a child’s assignment for them. [ 30 ] [ 31 ] [ 32 ] Read More
Con 2 Homework exacerbates the digital divide or homework gap. Kiara Taylor, financial expert, defined the digital divide as “the gap between demographics and regions that have access to modern information and communications technology and those that don’t. Though the term now encompasses the technical and financial ability to utilize available technology—along with access (or a lack of access) to the Internet—the gap it refers to is constantly shifting with the development of technology.” For students, this is often called the homework gap. [ 50 ] [ 51 ] 30% (about 15 to 16 million) public school students either did not have an adequate internet connection or an appropriate device, or both, for distance learning. Completing homework for these students is more complicated (having to find a safe place with an internet connection, or borrowing a laptop, for example) or impossible. [ 51 ] A Hispanic Heritage Foundation study found that 96.5% of students across the country needed to use the internet for homework, and nearly half reported they were sometimes unable to complete their homework due to lack of access to the internet or a computer, which often resulted in lower grades. [ 37 ] [ 38 ] One study concluded that homework increases social inequality because it “potentially serves as a mechanism to further advantage those students who already experience some privilege in the school system while further disadvantaging those who may already be in a marginalized position.” [ 39 ] Read More
Con 3 Homework does not help younger students, and may not help high school students. We’ve known for a while that homework does not help elementary students. A 2006 study found that “homework had no association with achievement gains” when measured by standardized tests results or grades. [ 7 ] Fourth grade students who did no homework got roughly the same score on the National Assessment of Educational Progress (NAEP) math exam as those who did 30 minutes of homework a night. Students who did 45 minutes or more of homework a night actually did worse. [ 41 ] Temple University professor Kathryn Hirsh-Pasek said that homework is not the most effective tool for young learners to apply new information: “They’re learning way more important skills when they’re not doing their homework.” [ 42 ] In fact, homework may not be helpful at the high school level either. Alfie Kohn, author of The Homework Myth, stated, “I interviewed high school teachers who completely stopped giving homework and there was no downside, it was all upside.” He explains, “just because the same kids who get more homework do a little better on tests, doesn’t mean the homework made that happen.” [ 52 ] Read More
Discussion Questions
1. Is homework beneficial? Consider the study data, your personal experience, and other types of information. Explain your answer(s).
2. If homework were banned, what other educational strategies would help students learn classroom material? Explain your answer(s).
3. How has homework been helpful to you personally? How has homework been unhelpful to you personally? Make carefully considered lists for both sides.
Take Action
1. Examine an argument in favor of quality homework assignments from Janine Bempechat.
2. Explore Oxford Learning’s infographic on the effects of homework on students.
3. Consider Joseph Lathan’s argument that homework promotes inequality .
4. Consider how you felt about the issue before reading this article. After reading the pros and cons on this topic, has your thinking changed? If so, how? List two to three ways. If your thoughts have not changed, list two to three ways your better understanding of the “other side of the issue” now helps you better argue your position.
5. Push for the position and policies you support by writing US national senators and representatives .
| 1. | Tom Loveless, “Homework in America: Part II of the 2014 Brown Center Report of American Education,” brookings.edu, Mar. 18, 2014 | |
| 2. | Edward Bok, “A National Crime at the Feet of American Parents,” , Jan. 1900 | |
| 3. | Tim Walker, “The Great Homework Debate: What’s Getting Lost in the Hype,” neatoday.org, Sep. 23, 2015 | |
| 4. | University of Phoenix College of Education, “Homework Anxiety: Survey Reveals How Much Homework K-12 Students Are Assigned and Why Teachers Deem It Beneficial,” phoenix.edu, Feb. 24, 2014 | |
| 5. | Organization for Economic Cooperation and Development (OECD), “PISA in Focus No. 46: Does Homework Perpetuate Inequities in Education?,” oecd.org, Dec. 2014 | |
| 6. | Adam V. Maltese, Robert H. Tai, and Xitao Fan, “When is Homework Worth the Time?: Evaluating the Association between Homework and Achievement in High School Science and Math,” , 2012 | |
| 7. | Harris Cooper, Jorgianne Civey Robinson, and Erika A. Patall, “Does Homework Improve Academic Achievement? A Synthesis of Researcher, 1987-2003,” , 2006 | |
| 8. | Gökhan Bas, Cihad Sentürk, and Fatih Mehmet Cigerci, “Homework and Academic Achievement: A Meta-Analytic Review of Research,” , 2017 | |
| 9. | Huiyong Fan, Jianzhong Xu, Zhihui Cai, Jinbo He, and Xitao Fan, “Homework and Students’ Achievement in Math and Science: A 30-Year Meta-Analysis, 1986-2015,” , 2017 | |
| 10. | Charlene Marie Kalenkoski and Sabrina Wulff Pabilonia, “Does High School Homework Increase Academic Achievement?,” iza.og, Apr. 2014 | |
| 11. | Ron Kurtus, “Purpose of Homework,” school-for-champions.com, July 8, 2012 | |
| 12. | Harris Cooper, “Yes, Teachers Should Give Homework – The Benefits Are Many,” newsobserver.com, Sep. 2, 2016 | |
| 13. | Tammi A. Minke, “Types of Homework and Their Effect on Student Achievement,” repository.stcloudstate.edu, 2017 | |
| 14. | LakkshyaEducation.com, “How Does Homework Help Students: Suggestions From Experts,” LakkshyaEducation.com (accessed Aug. 29, 2018) | |
| 15. | University of Montreal, “Do Kids Benefit from Homework?,” teaching.monster.com (accessed Aug. 30, 2018) | |
| 16. | Glenda Faye Pryor-Johnson, “Why Homework Is Actually Good for Kids,” memphisparent.com, Feb. 1, 2012 | |
| 17. | Joan M. Shepard, “Developing Responsibility for Completing and Handing in Daily Homework Assignments for Students in Grades Three, Four, and Five,” eric.ed.gov, 1999 | |
| 18. | Darshanand Ramdass and Barry J. Zimmerman, “Developing Self-Regulation Skills: The Important Role of Homework,” , 2011 | |
| 19. | US Department of Education, “Let’s Do Homework!,” ed.gov (accessed Aug. 29, 2018) | |
| 20. | Loretta Waldman, “Sociologist Upends Notions about Parental Help with Homework,” phys.org, Apr. 12, 2014 | |
| 21. | Frances L. Van Voorhis, “Reflecting on the Homework Ritual: Assignments and Designs,” , June 2010 | |
| 22. | Roel J. F. J. Aries and Sofie J. Cabus, “Parental Homework Involvement Improves Test Scores? A Review of the Literature,” , June 2015 | |
| 23. | Jamie Ballard, “40% of People Say Elementary School Students Have Too Much Homework,” yougov.com, July 31, 2018 | |
| 24. | Stanford University, “Stanford Survey of Adolescent School Experiences Report: Mira Costa High School, Winter 2017,” stanford.edu, 2017 | |
| 25. | Cathy Vatterott, “Rethinking Homework: Best Practices That Support Diverse Needs,” ascd.org, 2009 | |
| 26. | End the Race, “Homework: You Can Make a Difference,” racetonowhere.com (accessed Aug. 24, 2018) | |
| 27. | Elissa Strauss, “Opinion: Your Kid Is Right, Homework Is Pointless. Here’s What You Should Do Instead.,” cnn.com, Jan. 28, 2020 | |
| 28. | Jeanne Fratello, “Survey: Homework Is Biggest Source of Stress for Mira Costa Students,” digmb.com, Dec. 15, 2017 | |
| 29. | Clifton B. Parker, “Stanford Research Shows Pitfalls of Homework,” stanford.edu, Mar. 10, 2014 | |
| 30. | AdCouncil, “Cheating Is a Personal Foul: Academic Cheating Background,” glass-castle.com (accessed Aug. 16, 2018) | |
| 31. | Jeffrey R. Young, “High-Tech Cheating Abounds, and Professors Bear Some Blame,” chronicle.com, Mar. 28, 2010 | |
| 32. | Robin McClure, “Do You Do Your Child’s Homework?,” verywellfamily.com, Mar. 14, 2018 | |
| 33. | Robert M. Pressman, David B. Sugarman, Melissa L. Nemon, Jennifer, Desjarlais, Judith A. Owens, and Allison Schettini-Evans, “Homework and Family Stress: With Consideration of Parents’ Self Confidence, Educational Level, and Cultural Background,” , 2015 | |
| 34. | Heather Koball and Yang Jiang, “Basic Facts about Low-Income Children,” nccp.org, Jan. 2018 | |
| 35. | Meagan McGovern, “Homework Is for Rich Kids,” huffingtonpost.com, Sep. 2, 2016 | |
| 36. | H. Richard Milner IV, “Not All Students Have Access to Homework Help,” nytimes.com, Nov. 13, 2014 | |
| 37. | Claire McLaughlin, “The Homework Gap: The ‘Cruelest Part of the Digital Divide’,” neatoday.org, Apr. 20, 2016 | |
| 38. | Doug Levin, “This Evening’s Homework Requires the Use of the Internet,” edtechstrategies.com, May 1, 2015 | |
| 39. | Amy Lutz and Lakshmi Jayaram, “Getting the Homework Done: Social Class and Parents’ Relationship to Homework,” , June 2015 | |
| 40. | Sandra L. Hofferth and John F. Sandberg, “How American Children Spend Their Time,” psc.isr.umich.edu, Apr. 17, 2000 | |
| 41. | Alfie Kohn, “Does Homework Improve Learning?,” alfiekohn.org, 2006 | |
| 42. | Patrick A. Coleman, “Elementary School Homework Probably Isn’t Good for Kids,” fatherly.com, Feb. 8, 2018 | |
| 43. | Valerie Strauss, “Why This Superintendent Is Banning Homework – and Asking Kids to Read Instead,” washingtonpost.com, July 17, 2017 | |
| 44. | Pew Research Center, “The Way U.S. Teens Spend Their Time Is Changing, but Differences between Boys and Girls Persist,” pewresearch.org, Feb. 20, 2019 | |
| 45. | ThroughEducation, “The History of Homework: Why Was It Invented and Who Was behind It?,” , Feb. 14, 2020 | |
| 46. | History, “Why Homework Was Banned,” (accessed Feb. 24, 2022) | |
| 47. | Valerie Strauss, “Does Homework Work When Kids Are Learning All Day at Home?,” , Sep. 2, 2020 | |
| 48. | Sara M Moniuszko, “Is It Time to Get Rid of Homework? Mental Health Experts Weigh In,” , Aug. 17, 2021 | |
| 49. | Abby Freireich and Brian Platzer, “The Worsening Homework Problem,” , Apr. 13, 2021 | |
| 50. | Kiara Taylor, “Digital Divide,” , Feb. 12, 2022 | |
| 51. | Marguerite Reardon, “The Digital Divide Has Left Millions of School Kids Behind,” , May 5, 2021 | |
| 52. | Rachel Paula Abrahamson, “Why More and More Teachers Are Joining the Anti-Homework Movement,” , Sep. 10, 2021 |
More School Debate Topics
Should K-12 Students Dissect Animals in Science Classrooms? – Proponents say dissecting real animals is a better learning experience. Opponents say the practice is bad for the environment.
Should Students Have to Wear School Uniforms? – Proponents say uniforms may increase student safety. Opponents say uniforms restrict expression.
Should Corporal Punishment Be Used in K-12 Schools? – Proponents say corporal punishment is an appropriate discipline. Opponents say it inflicts long-lasting physical and mental harm on students.
ProCon/Encyclopaedia Britannica, Inc. 325 N. LaSalle Street, Suite 200 Chicago, Illinois 60654 USA
Natalie Leppard Managing Editor [email protected]
© 2023 Encyclopaedia Britannica, Inc. All rights reserved
- Social Media
- Death Penalty
- School Uniforms
- Video Games
- Animal Testing
- Gun Control
- Banned Books
- Teachers’ Corner
Cite This Page
ProCon.org is the institutional or organization author for all ProCon.org pages. Proper citation depends on your preferred or required style manual. Below are the proper citations for this page according to four style manuals (in alphabetical order): the Modern Language Association Style Manual (MLA), the Chicago Manual of Style (Chicago), the Publication Manual of the American Psychological Association (APA), and Kate Turabian's A Manual for Writers of Term Papers, Theses, and Dissertations (Turabian). Here are the proper bibliographic citations for this page according to four style manuals (in alphabetical order):
[Editor's Note: The APA citation style requires double spacing within entries.]
[Editor’s Note: The MLA citation style requires double spacing within entries.]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
The effect of physical activity homework on physical activity among college students
Affiliation.
- 1 Department of Health, Physical Education, and Recreation, Western Carolina University Cullowhee, NC 28723, USA.
- PMID: 19420398
- DOI: 10.1123/jpah.6.2.203
Background: This study examined the effect of using physical activity homework on physical activity levels of college students.
Methods: Students in randomly assigned sections of a university health course were assigned 30 minutes of physical activity homework 3 days a week or no homework for 12 weeks. Participants completed self-reports of physical activity before the homework intervention and again at the conclusion of the 12 weeks of physical activity homework.
Results: Participants in all course sections reported significant increases in the number of days per week of moderate and vigorous physical activity. Participants in homework sections additionally showed significant increases in the days they engaged in muscular strength/endurance training and activities to manage weight. Participants in sections without homework showed a significant increase in the number of days engaged in flexibility training. Comparison of gain scores showed statistically significant increases by the homework group in the days they participated in activities designed to manage weight.
Conclusion: Physical activity homework was deemed to be an effective method of increasing college students' levels of physical activity.
PubMed Disclaimer
Similar articles
- Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study. Duncan S, McPhee JC, Schluter PJ, Zinn C, Smith R, Schofield G. Duncan S, et al. Int J Behav Nutr Phys Act. 2011 Nov 15;8:127. doi: 10.1186/1479-5868-8-127. Int J Behav Nutr Phys Act. 2011. PMID: 22085440 Free PMC article. Clinical Trial.
- The Effect of Chinese Traditional Exercise-Baduanjin on Physical and Psychological Well-Being of College Students: A Randomized Controlled Trial. Li M, Fang Q, Li J, Zheng X, Tao J, Yan X, Lin Q, Lan X, Chen B, Zheng G, Chen L. Li M, et al. PLoS One. 2015 Jul 9;10(7):e0130544. doi: 10.1371/journal.pone.0130544. eCollection 2015. PLoS One. 2015. PMID: 26158769 Free PMC article. Clinical Trial.
- Wellness and resilience for college and beyond: protocol for a quasi-experimental pilot study investigating a dialectical behaviour therapy skill-infused college course. Chugani CD, Fuhrman B, Abebe KZ, Talis J, Miller E, Coulter RWS. Chugani CD, et al. BMJ Open. 2020 Jun 21;10(6):e036833. doi: 10.1136/bmjopen-2020-036833. BMJ Open. 2020. PMID: 32565475 Free PMC article.
- Impact of an online healthful eating and physical activity program for college students. Greene GW, White AA, Hoerr SL, Lohse B, Schembre SM, Riebe D, Patterson J, Kattelmann KK, Shoff S, Horacek T, Blissmer B, Phillips BW. Greene GW, et al. Am J Health Promot. 2012 Nov-Dec;27(2):e47-58. doi: 10.4278/ajhp.110606-QUAN-239. Am J Health Promot. 2012. PMID: 23113786 Clinical Trial.
- Assessment of weight status, dietary habits and beliefs, physical activity, and nutritional knowledge among university students. Yahia N, Wang D, Rapley M, Dey R. Yahia N, et al. Perspect Public Health. 2016 Jul;136(4):231-44. doi: 10.1177/1757913915609945. Epub 2015 Oct 16. Perspect Public Health. 2016. PMID: 26475773 Review.
- Fitness Promotion in a Jump Rope-Based Homework Intervention for Middle School Students: A Randomized Controlled Trial. Huang F, Song Y, Zhao Y, Han Y, Fang Q. Huang F, et al. Front Psychol. 2022 Jun 16;13:912635. doi: 10.3389/fpsyg.2022.912635. eCollection 2022. Front Psychol. 2022. PMID: 35783780 Free PMC article.
- Types of Interventions Targeting Dietary, Physical Activity, and Weight-Related Outcomes among University Students: A Systematic Review of Systematic Reviews. Belogianni K, Baldwin C. Belogianni K, et al. Adv Nutr. 2019 Sep 1;10(5):848-863. doi: 10.1093/advances/nmz027. Adv Nutr. 2019. PMID: 31181143 Free PMC article.
- Effectiveness of interventions targeting physical activity, nutrition and healthy weight for university and college students: a systematic review and meta-analysis. Plotnikoff RC, Costigan SA, Williams RL, Hutchesson MJ, Kennedy SG, Robards SL, Allen J, Collins CE, Callister R, Germov J. Plotnikoff RC, et al. Int J Behav Nutr Phys Act. 2015 Apr 1;12:45. doi: 10.1186/s12966-015-0203-7. Int J Behav Nutr Phys Act. 2015. PMID: 25890337 Free PMC article. Review.
- Interventions for weight gain prevention during the transition to young adulthood: a review of the literature. Laska MN, Pelletier JE, Larson NI, Story M. Laska MN, et al. J Adolesc Health. 2012 Apr;50(4):324-33. doi: 10.1016/j.jadohealth.2012.01.016. J Adolesc Health. 2012. PMID: 22443834 Free PMC article. Review.
Publication types
- Search in MeSH
LinkOut - more resources
Full text sources.
- Sheridan PubFactory

- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
Along with Stanford news and stories, show me:
- Student information
- Faculty/Staff information
We want to provide announcements, events, leadership messages and resources that are relevant to you. Your selection is stored in a browser cookie which you can remove at any time using “Clear all personalization” below.

Education scholar Denise Pope has found that too much homework has negative effects on student well-being and behavioral engagement. (Image credit: L.A. Cicero)
A Stanford researcher found that too much homework can negatively affect kids, especially their lives away from school, where family, friends and activities matter.
“Our findings on the effects of homework challenge the traditional assumption that homework is inherently good,” wrote Denise Pope , a senior lecturer at the Stanford Graduate School of Education and a co-author of a study published in the Journal of Experimental Education .
The researchers used survey data to examine perceptions about homework, student well-being and behavioral engagement in a sample of 4,317 students from 10 high-performing high schools in upper-middle-class California communities. Along with the survey data, Pope and her colleagues used open-ended answers to explore the students’ views on homework.
Median household income exceeded $90,000 in these communities, and 93 percent of the students went on to college, either two-year or four-year.
Students in these schools average about 3.1 hours of homework each night.
“The findings address how current homework practices in privileged, high-performing schools sustain students’ advantage in competitive climates yet hinder learning, full engagement and well-being,” Pope wrote.
Pope and her colleagues found that too much homework can diminish its effectiveness and even be counterproductive. They cite prior research indicating that homework benefits plateau at about two hours per night, and that 90 minutes to two and a half hours is optimal for high school.
Their study found that too much homework is associated with:
* Greater stress: 56 percent of the students considered homework a primary source of stress, according to the survey data. Forty-three percent viewed tests as a primary stressor, while 33 percent put the pressure to get good grades in that category. Less than 1 percent of the students said homework was not a stressor.
* Reductions in health: In their open-ended answers, many students said their homework load led to sleep deprivation and other health problems. The researchers asked students whether they experienced health issues such as headaches, exhaustion, sleep deprivation, weight loss and stomach problems.
* Less time for friends, family and extracurricular pursuits: Both the survey data and student responses indicate that spending too much time on homework meant that students were “not meeting their developmental needs or cultivating other critical life skills,” according to the researchers. Students were more likely to drop activities, not see friends or family, and not pursue hobbies they enjoy.
A balancing act
The results offer empirical evidence that many students struggle to find balance between homework, extracurricular activities and social time, the researchers said. Many students felt forced or obligated to choose homework over developing other talents or skills.
Also, there was no relationship between the time spent on homework and how much the student enjoyed it. The research quoted students as saying they often do homework they see as “pointless” or “mindless” in order to keep their grades up.
“This kind of busy work, by its very nature, discourages learning and instead promotes doing homework simply to get points,” Pope said.
She said the research calls into question the value of assigning large amounts of homework in high-performing schools. Homework should not be simply assigned as a routine practice, she said.
“Rather, any homework assigned should have a purpose and benefit, and it should be designed to cultivate learning and development,” wrote Pope.
High-performing paradox
In places where students attend high-performing schools, too much homework can reduce their time to foster skills in the area of personal responsibility, the researchers concluded. “Young people are spending more time alone,” they wrote, “which means less time for family and fewer opportunities to engage in their communities.”
Student perspectives
The researchers say that while their open-ended or “self-reporting” methodology to gauge student concerns about homework may have limitations – some might regard it as an opportunity for “typical adolescent complaining” – it was important to learn firsthand what the students believe.
The paper was co-authored by Mollie Galloway from Lewis and Clark College and Jerusha Conner from Villanova University.
Media Contacts
Denise Pope, Stanford Graduate School of Education: (650) 725-7412, [email protected] Clifton B. Parker, Stanford News Service: (650) 725-0224, [email protected]
Does homework really work?
by: Leslie Crawford | Updated: December 12, 2023
Print article

You know the drill. It’s 10:15 p.m., and the cardboard-and-toothpick Golden Gate Bridge is collapsing. The pages of polynomials have been abandoned. The paper on the Battle of Waterloo seems to have frozen in time with Napoleon lingering eternally over his breakfast at Le Caillou. Then come the tears and tantrums — while we parents wonder, Does the gain merit all this pain? Is this just too much homework?
However the drama unfolds night after night, year after year, most parents hold on to the hope that homework (after soccer games, dinner, flute practice, and, oh yes, that childhood pastime of yore known as playing) advances their children academically.
But what does homework really do for kids? Is the forest’s worth of book reports and math and spelling sheets the average American student completes in their 12 years of primary schooling making a difference? Or is it just busywork?
Homework haterz
Whether or not homework helps, or even hurts, depends on who you ask. If you ask my 12-year-old son, Sam, he’ll say, “Homework doesn’t help anything. It makes kids stressed-out and tired and makes them hate school more.”
Nothing more than common kid bellyaching?
Maybe, but in the fractious field of homework studies, it’s worth noting that Sam’s sentiments nicely synopsize one side of the ivory tower debate. Books like The End of Homework , The Homework Myth , and The Case Against Homework the film Race to Nowhere , and the anguished parent essay “ My Daughter’s Homework is Killing Me ” make the case that homework, by taking away precious family time and putting kids under unneeded pressure, is an ineffective way to help children become better learners and thinkers.
One Canadian couple took their homework apostasy all the way to the Supreme Court of Canada. After arguing that there was no evidence that it improved academic performance, they won a ruling that exempted their two children from all homework.
So what’s the real relationship between homework and academic achievement?
How much is too much?
To answer this question, researchers have been doing their homework on homework, conducting and examining hundreds of studies. Chris Drew Ph.D., founder and editor at The Helpful Professor recently compiled multiple statistics revealing the folly of today’s after-school busy work. Does any of the data he listed below ring true for you?
• 45 percent of parents think homework is too easy for their child, primarily because it is geared to the lowest standard under the Common Core State Standards .
• 74 percent of students say homework is a source of stress , defined as headaches, exhaustion, sleep deprivation, weight loss, and stomach problems.
• Students in high-performing high schools spend an average of 3.1 hours a night on homework , even though 1 to 2 hours is the optimal duration, according to a peer-reviewed study .
Not included in the list above is the fact many kids have to abandon activities they love — like sports and clubs — because homework deprives them of the needed time to enjoy themselves with other pursuits.
Conversely, The Helpful Professor does list a few pros of homework, noting it teaches discipline and time management, and helps parents know what’s being taught in the class.
The oft-bandied rule on homework quantity — 10 minutes a night per grade (starting from between 10 to 20 minutes in first grade) — is listed on the National Education Association’s website and the National Parent Teacher Association’s website , but few schools follow this rule.
Do you think your child is doing excessive homework? Harris Cooper Ph.D., author of a meta-study on homework , recommends talking with the teacher. “Often there is a miscommunication about the goals of homework assignments,” he says. “What appears to be problematic for kids, why they are doing an assignment, can be cleared up with a conversation.” Also, Cooper suggests taking a careful look at how your child is doing the assignments. It may seem like they’re taking two hours, but maybe your child is wandering off frequently to get a snack or getting distracted.
Less is often more
If your child is dutifully doing their work but still burning the midnight oil, it’s worth intervening to make sure your child gets enough sleep. A 2012 study of 535 high school students found that proper sleep may be far more essential to brain and body development.
For elementary school-age children, Cooper’s research at Duke University shows there is no measurable academic advantage to homework. For middle-schoolers, Cooper found there is a direct correlation between homework and achievement if assignments last between one to two hours per night. After two hours, however, achievement doesn’t improve. For high schoolers, Cooper’s research suggests that two hours per night is optimal. If teens have more than two hours of homework a night, their academic success flatlines. But less is not better. The average high school student doing homework outperformed 69 percent of the students in a class with no homework.
Many schools are starting to act on this research. A Florida superintendent abolished homework in her 42,000 student district, replacing it with 20 minutes of nightly reading. She attributed her decision to “ solid research about what works best in improving academic achievement in students .”
More family time
A 2020 survey by Crayola Experience reports 82 percent of children complain they don’t have enough quality time with their parents. Homework deserves much of the blame. “Kids should have a chance to just be kids and do things they enjoy, particularly after spending six hours a day in school,” says Alfie Kohn, author of The Homework Myth . “It’s absurd to insist that children must be engaged in constructive activities right up until their heads hit the pillow.”
By far, the best replacement for homework — for both parents and children — is bonding, relaxing time together.
Homes Nearby
Homes for rent and sale near schools

How families of color can fight for fair discipline in school

Dealing with teacher bias

The most important school data families of color need to consider
Yes! Sign me up for updates relevant to my child's grade.
Please enter a valid email address
Thank you for signing up!
Server Issue: Please try again later. Sorry for the inconvenience
share this!
August 16, 2021
Is it time to get rid of homework? Mental health experts weigh in
by Sara M Moniuszko

It's no secret that kids hate homework. And as students grapple with an ongoing pandemic that has had a wide-range of mental health impacts, is it time schools start listening to their pleas over workloads?
Some teachers are turning to social media to take a stand against homework .
Tiktok user @misguided.teacher says he doesn't assign it because the "whole premise of homework is flawed."
For starters, he says he can't grade work on "even playing fields" when students' home environments can be vastly different.
"Even students who go home to a peaceful house, do they really want to spend their time on busy work? Because typically that's what a lot of homework is, it's busy work," he says in the video that has garnered 1.6 million likes. "You only get one year to be 7, you only got one year to be 10, you only get one year to be 16, 18."
Mental health experts agree heavy work loads have the potential do more harm than good for students, especially when taking into account the impacts of the pandemic. But they also say the answer may not be to eliminate homework altogether.
Emmy Kang, mental health counselor at Humantold, says studies have shown heavy workloads can be "detrimental" for students and cause a "big impact on their mental, physical and emotional health."
"More than half of students say that homework is their primary source of stress, and we know what stress can do on our bodies," she says, adding that staying up late to finish assignments also leads to disrupted sleep and exhaustion.
Cynthia Catchings, a licensed clinical social worker and therapist at Talkspace, says heavy workloads can also cause serious mental health problems in the long run, like anxiety and depression.
And for all the distress homework causes, it's not as useful as many may think, says Dr. Nicholas Kardaras, a psychologist and CEO of Omega Recovery treatment center.
"The research shows that there's really limited benefit of homework for elementary age students, that really the school work should be contained in the classroom," he says.
For older students, Kang says homework benefits plateau at about two hours per night.
"Most students, especially at these high-achieving schools, they're doing a minimum of three hours, and it's taking away time from their friends from their families, their extracurricular activities. And these are all very important things for a person's mental and emotional health."
Catchings, who also taught third to 12th graders for 12 years, says she's seen the positive effects of a no homework policy while working with students abroad.
"Not having homework was something that I always admired from the French students (and) the French schools, because that was helping the students to really have the time off and really disconnect from school ," she says.
The answer may not be to eliminate homework completely, but to be more mindful of the type of work students go home with, suggests Kang, who was a high-school teacher for 10 years.
"I don't think (we) should scrap homework, I think we should scrap meaningless, purposeless busy work-type homework. That's something that needs to be scrapped entirely," she says, encouraging teachers to be thoughtful and consider the amount of time it would take for students to complete assignments.
The pandemic made the conversation around homework more crucial
Mindfulness surrounding homework is especially important in the context of the last two years. Many students will be struggling with mental health issues that were brought on or worsened by the pandemic, making heavy workloads even harder to balance.
"COVID was just a disaster in terms of the lack of structure. Everything just deteriorated," Kardaras says, pointing to an increase in cognitive issues and decrease in attention spans among students. "School acts as an anchor for a lot of children, as a stabilizing force, and that disappeared."
But even if students transition back to the structure of in-person classes, Kardaras suspects students may still struggle after two school years of shifted schedules and disrupted sleeping habits.
"We've seen adults struggling to go back to in-person work environments from remote work environments. That effect is amplified with children because children have less resources to be able to cope with those transitions than adults do," he explains.
'Get organized' ahead of back-to-school
In order to make the transition back to in-person school easier, Kang encourages students to "get good sleep, exercise regularly (and) eat a healthy diet."
To help manage workloads, she suggests students "get organized."
"There's so much mental clutter up there when you're disorganized... sitting down and planning out their study schedules can really help manage their time," she says.
Breaking assignments up can also make things easier to tackle.
"I know that heavy workloads can be stressful, but if you sit down and you break down that studying into smaller chunks, they're much more manageable."
If workloads are still too much, Kang encourages students to advocate for themselves.
"They should tell their teachers when a homework assignment just took too much time or if it was too difficult for them to do on their own," she says. "It's good to speak up and ask those questions. Respectfully, of course, because these are your teachers. But still, I think sometimes teachers themselves need this feedback from their students."
©2021 USA Today Distributed by Tribune Content Agency, LLC.
Explore further
Feedback to editors

Genomics reveals sled dogs' Siberian lineage
2 hours ago

Tech billionaire returns to Earth after first private spacewalk
3 hours ago

Saturday Citations: Permian-Triassic mystery solved; cute baby sighted; the nine-day 2023 seismic event
22 hours ago

Researchers develop novel covalent organic frameworks for precise cancer treatment delivery
Sep 13, 2024

Flowers use adjustable 'paint by numbers' petal designs to attract pollinators, researchers discover

Astronomers discover new planet in Great Bear constellation

Device malfunctions from continuous current lead to discovery that can improve design of microelectronic devices

Soil pH drives microbial community composition: Study shows how bacteria work together to thrive in difficult conditions

Gravity study gives insights into hidden features beneath lost ocean of Mars and rising Olympus Mons

Technique to study how proteins bind to DNA is easily misused: Researchers offer a solution
Relevant physicsforums posts, how to explain bell's theorem to non-scientists, i want to start tutoring online -- looking for advice, are excuses for academic parties getting thinner or is it just me.
Sep 7, 2024
AAPT 2024 Summer Meeting Boston, MA (July 2024) - are you going?
Sep 2, 2024
RIP Edward "Joe" Redish (1942 - 2024), Physics Education
Incandescent bulbs in teaching.
Aug 21, 2024
More from STEM Educators and Teaching
Related Stories

Smartphones are lowering student's grades, study finds
Aug 18, 2020

Doing homework is associated with change in students' personality
Oct 6, 2017

Scholar suggests ways to craft more effective homework assignments
Oct 1, 2015

Should parents help their kids with homework?
Aug 29, 2019

How much math, science homework is too much?
Mar 23, 2015

Anxiety, depression, burnout rising as college students prepare to return to campus
Jul 26, 2021
Recommended for you

Virtual learning linked to rise in chronic absenteeism, study finds
Sep 5, 2024

AI tools like ChatGPT popular among students who struggle with concentration and attention
Aug 28, 2024

Researchers find academic equivalent of a Great Gatsby Curve in science mentorships
Aug 27, 2024

More academic freedom leads to more innovation, reports study

Statistical analysis can detect when ChatGPT is used to cheat on multiple-choice chemistry exams
Aug 14, 2024

Larger teams in academic research worsen career prospects, study finds
Let us know if there is a problem with our content.
Use this form if you have come across a typo, inaccuracy or would like to send an edit request for the content on this page. For general inquiries, please use our contact form . For general feedback, use the public comments section below (please adhere to guidelines ).
Please select the most appropriate category to facilitate processing of your request
Thank you for taking time to provide your feedback to the editors.
Your feedback is important to us. However, we do not guarantee individual replies due to the high volume of messages.
E-mail the story
Your email address is used only to let the recipient know who sent the email. Neither your address nor the recipient's address will be used for any other purpose. The information you enter will appear in your e-mail message and is not retained by Phys.org in any form.
Newsletter sign up
Get weekly and/or daily updates delivered to your inbox. You can unsubscribe at any time and we'll never share your details to third parties.
More information Privacy policy
Donate and enjoy an ad-free experience
We keep our content available to everyone. Consider supporting Science X's mission by getting a premium account.
E-mail newsletter
You are using an outdated browser. Please upgrade your browser or activate Google Chrome Frame to improve your experience.
Homework or Personal Lives?
Many students get home and the first thing they do is homework. They’re pressured by their parents to do their homework while simultaneously being encouraged to spend time with family, eat, spend time with friends, go outside, participate in sports or other extracurricular activities, and sleep for 7+ hours. Rather than motivating students to master material and learn efficiently, homework negatively impacts students by taking away from personal time that is necessary for them to lead balanced lives.
In an article published by The Washington Post by Gerald K LeTendre, a professor of education in education policy studies at Penn State, states that, “Worldwide, homework is not associated with high national levels of academic achievement.” This means that there is no direct correlation between homework and test grades, and very few studies have been able to prove this, and the ones that have were more of a reach. At Science Leadership Academy in Philadelphia, 16 out of 19 of the students in Fire Stream agreed that homework adds extra stress onto them or takes time away from other things that they’re encouraged to do, such as sports, extra classes, extracurricular activities, family time, etc. This means that just over 84% of students in Fire Stream have agreed that homework is added stress and takes time away from things that they’re encouraged to do outside of school. Many students participate in these activities because they’re passionate about them and it makes them happy. Sports and exercise is proven to relieve stress, homework adds stress and if time for this stress reliever is taken away that just means more stress, this can cause more problems in many aspects of their lives.
In an article written by CNN about how homework has been banned in some cities and not others, “What is clear is that parents and kids don't live in the world of academic research; they live in the real world where there are piles of homework on the kitchen table.” Meaning that students don’t have the luxury of just easily saying that homework helps their academic performance or not, and they don’t have the luxury of just not doing homework. That is especially true to highschool students who have to regularly chose between sleep and doing work, especially when they get homework from every class every night and homework can be up to 30% of their grade. Students in every grade get piles of homework and a lot of the time they don’t have resources on hand to see if they’re right or to get help, meaning they might do it wrong and not learn anything at all. Even if students do try and do their homework it might take a while, according to Nationwide Children’s Hospital adolescents should be getting 9 to 9 ½ hours of sleep per night. Due to homework and trying to fit other after school activities in many adolescents don’t get the necessary amount of sleep. Sleep deprivation in teens has many negative effects such as mood changes, being more inclined to engage in risky behavior such as driving fast, drinking, etc, doing worse in school, and declined cognitive abilities.
In an article published by the New York Times, a mother explained how… , “The stress homework places on families starts early.” The article also talks about how homework takes away from family time and family activities. The author also says that her kids “are fighting not just over the homework, but also over their share of my coveted attention and my unique ability to download and print images.” This shows how homework adds extra pressure and can cause tension in families. It takes away from family time and causes more stress on students and parents. It’s almost as if once children start school and the homework starts that it never stops, and that more family time is taken away while more stress is added.
In a study concluded in 2003 by Dr. Harris Cooper he tries to argue that homework has a positive effect on students, but his studies also found no direct correlation between increased homework for students and improved test scores. Cooper himself said that “The analysis also showed that too much homework can be counter-productive for students at all levels.” Meaning that excessive amounts of homework can cause negative effects on students, but who is judging what excessive amounts of homework means? He talks about the “10 minute rule” meaning that every grade that a student increases they should get 10 more minutes of homework, meaning that a second grader should get 20 minutes, and a twelfth grader should get around 2 hours of homework. That would seem ideal, but in most high school settings teachers don’t interact with each other to see how much homework each of them give to equal it out to around 2 hours. This means that one class’s homework could take a student 2 hours alone and that would be what the ideal amount of homework is, so if it takes 2 hours for one class’s homework then how are students supposed to have positive benefits from doing all of their homework? Cooper’s research was also limited because very little research was done to see if student’s race, socioeconomic status, or even their ability levels has an affect on how much homework is “good” for said age range. This means that other aspects than just that they’re students in a certain grade weren’t taken into consideration. These things could cause major changes to the data that was collected.
Rather than encouraging students to master material and learn efficiently, homework negatively impacts students and families by causing more stress and taking away from family time. This is a problem not just for the overworked students, but also for students who have more complex personal lives. Many students work or have family obligations that they have to deal with, but don’t necessarily feel comfortable talking to a teacher about them. Although teachers might not think that the amount of homework that they give matters much,its influence goes beyond giving students work to do at home to how they interact in other important personal aspects of their life.
Works Cited:
LeTendre, Gerald K. “Homework Could Have an Effect on Kids’ Health. Should Schools Ban It?” The Washington Post , WP Company, 2 Sept. 2015, www.washingtonpost.com/posteverything/wp/2015/09/02/homework-could-have-an-effect-on-kids-health-should-schools-ban-it/?utm_term=.3ed6d0fa2c72.
Kralovec, Etta. “Should Schools Ban Homework?” CNN , Cable News Network, 5 Sept. 2014, www.cnn.com/2014/09/05/opinion/kralovec-ban-homework/index.html.
Dell'Antonia, Kj. “Homework's Emotional Toll on Students and Families.” The New York Times , The New York Times, 12 Mar. 2014, parenting.blogs.nytimes.com/2014/03/12/homeworks-emotional-toll-on-students-and-families/.
“Duke Study: Homework Helps Students Succeed in School, As Long as There Isn't Too Much.” Duke Today , Duke Today, 7 Mar. 2006, today.duke.edu/2006/03/homework.html.
“Sleep in Adolescents (13-18 Years).” Sleep in Adolescents :: Nationwide Children's Hospital , www.nationwidechildrens.org/sleep-in-adolescents
Comments (1)

A question that I have after reading this is in what other ways can we as students improve our learning without homework?
This 2fer has changed my opinion about how much homework affects a student's life in a bad way more than a good way.
Log in to post a comment.
You can also log in with your email address.
Homework anxiety: Why it happens and how to help

By Gail Belsky
Expert reviewed by Jerome Schultz, PhD
Quick tips to help kids with homework anxiety
Quick tip 1, try self-calming strategies..

Try some deep breathing, gentle stretching, or a short walk before starting homework. These strategies can help reset the mind and relieve anxiety.
Quick tip 2
Set a time limit..

Give kids a set amount of time for homework to help it feel more manageable. Try using the “10-minute rule” that many schools use — that’s 10 minutes of homework per grade level. And let kids know it’s OK to stop working for the night.
Quick tip 3
Cut out distractions..
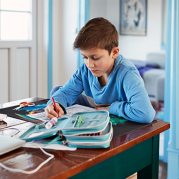
Have kids do homework in a quiet area. Turn off the TV, silence cell phones, and, if possible, limit people coming and going in the room or around the space.
Quick tip 4
Start with the easiest task..
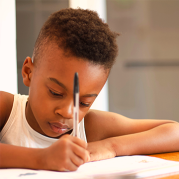
Try having kids do the easiest, quickest assignments first. That way, they’ll feel good about getting a task done — and may be less anxious about the rest of the homework.
Quick tip 5
Use a calm voice..

When kids feel anxious about homework, they might get angry, yell, or cry. Avoid matching their tone of voice. Take a deep breath and keep your voice steady and calm. Let them know you’re there for them.
Sometimes kids just don’t want to do homework. They complain, procrastinate, or rush through the work so they can do something fun. But for other kids, it’s not so simple. Homework may actually give them anxiety.
It’s not always easy to know when kids have homework anxiety. Some kids may share what they’re feeling when you ask. But others can’t yet identify what they’re feeling, or they're not willing to talk about it.
Homework anxiety often starts in early grade school. It can affect any child. But it’s an especially big issue for kids who are struggling in school. They may think they can’t do the work. Or they may not have the right support to get it done.
Keep in mind that some kids may seem anxious about homework but are actually anxious about something else. That’s why it’s important to keep track of when kids get anxious and what they were doing right before. The more you notice what’s happening, the better you can help.
Dive deeper
What homework anxiety looks like.
Kids with homework anxiety might:
Find excuses to avoid homework
Lie about homework being done
Get consistently angry about homework
Be moody or grumpy after school
Complain about not feeling well after school or before homework time
Cry easily or seem overly sensitive
Be afraid of making even small mistakes
Shut down and not want to talk after school
Say “I can’t do it!” before even trying
Learn about other homework challenges kids might be facing .
Why kids get homework anxiety
Kids with homework anxiety are often struggling with a specific skill. They might worry about falling behind their classmates. But there are other factors that cause homework anxiety:
Test prep: Homework that helps kids prepare for a test makes it sound very important. This can raise stress levels.
Perfectionism: Some kids who do really well in a subject may worry that their work “won’t be good enough.”
Trouble managing emotions: For kids who easily get flooded by emotions, homework can be a trigger for anxiety.
Too much homework: Sometimes kids are anxious because they have more work than they can handle.
Use this list to see if kids might have too much homework .
When kids are having homework anxiety, families, educators, and health care providers should work together to understand what’s happening. Start by sharing notes on what you’re seeing and look for patterns . By working together, you’ll develop a clearer sense of what’s going on and how to help.
Parents and caregivers: Start by asking questions to get your child to open up about school . But if kids are struggling with the work itself, they may not want to tell you. You’ll need to talk with your child’s teacher to get insight into what’s happening in school and find out if your child needs help in a specific area.
Explore related topics
- Share full article
Advertisement
Supported by
Student Opinion
Should We Get Rid of Homework?
Some educators are pushing to get rid of homework. Would that be a good thing?

By Jeremy Engle and Michael Gonchar
Do you like doing homework? Do you think it has benefited you educationally?
Has homework ever helped you practice a difficult skill — in math, for example — until you mastered it? Has it helped you learn new concepts in history or science? Has it helped to teach you life skills, such as independence and responsibility? Or, have you had a more negative experience with homework? Does it stress you out, numb your brain from busywork or actually make you fall behind in your classes?
Should we get rid of homework?
In “ The Movement to End Homework Is Wrong, ” published in July, the Times Opinion writer Jay Caspian Kang argues that homework may be imperfect, but it still serves an important purpose in school. The essay begins:
Do students really need to do their homework? As a parent and a former teacher, I have been pondering this question for quite a long time. The teacher side of me can acknowledge that there were assignments I gave out to my students that probably had little to no academic value. But I also imagine that some of my students never would have done their basic reading if they hadn’t been trained to complete expected assignments, which would have made the task of teaching an English class nearly impossible. As a parent, I would rather my daughter not get stuck doing the sort of pointless homework I would occasionally assign, but I also think there’s a lot of value in saying, “Hey, a lot of work you’re going to end up doing in your life is pointless, so why not just get used to it?” I certainly am not the only person wondering about the value of homework. Recently, the sociologist Jessica McCrory Calarco and the mathematics education scholars Ilana Horn and Grace Chen published a paper, “ You Need to Be More Responsible: The Myth of Meritocracy and Teachers’ Accounts of Homework Inequalities .” They argued that while there’s some evidence that homework might help students learn, it also exacerbates inequalities and reinforces what they call the “meritocratic” narrative that says kids who do well in school do so because of “individual competence, effort and responsibility.” The authors believe this meritocratic narrative is a myth and that homework — math homework in particular — further entrenches the myth in the minds of teachers and their students. Calarco, Horn and Chen write, “Research has highlighted inequalities in students’ homework production and linked those inequalities to differences in students’ home lives and in the support students’ families can provide.”
Mr. Kang argues:
But there’s a defense of homework that doesn’t really have much to do with class mobility, equality or any sense of reinforcing the notion of meritocracy. It’s one that became quite clear to me when I was a teacher: Kids need to learn how to practice things. Homework, in many cases, is the only ritualized thing they have to do every day. Even if we could perfectly equalize opportunity in school and empower all students not to be encumbered by the weight of their socioeconomic status or ethnicity, I’m not sure what good it would do if the kids didn’t know how to do something relentlessly, over and over again, until they perfected it. Most teachers know that type of progress is very difficult to achieve inside the classroom, regardless of a student’s background, which is why, I imagine, Calarco, Horn and Chen found that most teachers weren’t thinking in a structural inequalities frame. Holistic ideas of education, in which learning is emphasized and students can explore concepts and ideas, are largely for the types of kids who don’t need to worry about class mobility. A defense of rote practice through homework might seem revanchist at this moment, but if we truly believe that schools should teach children lessons that fall outside the meritocracy, I can’t think of one that matters more than the simple satisfaction of mastering something that you were once bad at. That takes homework and the acknowledgment that sometimes a student can get a question wrong and, with proper instruction, eventually get it right.
We are having trouble retrieving the article content.
Please enable JavaScript in your browser settings.
Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.
Thank you for your patience while we verify access.
Already a subscriber? Log in .
Want all of The Times? Subscribe .
How to Reduce Homework Stress
If homework is a source of frustration and stress in your home, it doesn’t have to be that way! Read on to learn effective strategies to reduce your child’s homework stress.

Author Katie Wickliff
Published March 2024
If homework is a source of frustration and stress in your home, it doesn’t have to be that way! Read on to learn effective strategies to reduce your child’s homework stress.
- Key takeaways
- Homework stress can be a significant problem for children and their families
- An appropriate amount of quality homework can be beneficial for students
- Parents can help reduce homework stress in several key ways
Table of contents
- Homework stress effects
- How to reduce homework stress
As a parent who has felt the frustration of watching my child be reduced to tears because of her homework each night, I’ve often wondered: do these math worksheets and reading trackers really make a difference to a child’s academic success? Or does homework cause stress without having a positive impact on learning?
If your child experiences a significant amount of homework stress, you may feel at a loss to help. However, there are several things you can do at home to minimize the negative effects of this stress on your child–and you! We’ve put together a list of research-based practices that can help your child better handle their homework load.
The Effects of Homework Stress on Students
Does homework cause stress? Short answer: Yes. It’s been well documented that too much homework can cause stress and anxiety for students–and their parents. However, do the benefits of homework outweigh the costs? Is homework “worth” the frustration and exhaustion that our children experience?
Findings on the benefits of homework at the elementary school level are mixed, with studies showing that homework appears to have more positive effects under certain conditions for certain groups of students.
After examining decades of studies on the relationship between homework and academic achievement, leading homework researcher Harris M. Cooper has proposed the “10-minute rule,” suggesting that homework be limited to 10 minutes per grade level. For example, children in 3rd grade should do no more than 30 minutes of homework daily, while a 1st grader should do no more than 10 minutes of homework. The National Parent Teacher Association and the National Education Association both endorse this guideline as a general rule of thumb.
Because of these research findings, Doodle believes that an appropriate amount of quality homework can help students feel more positive about learning and can provide parents with a critical connection to their child’s school experience . But to keep learning positive, we need to reduce the amount of stress both students and parents feel about homework.
1. Routine, Routine, Routine
Creating an after-school routine and sticking to it helps children feel organized, but with sports, tutoring, or music lessons, many children have varying weekday schedules. As a former classroom teacher and private tutor, I suggest that families post a weekly schedule somewhere visible and communicate that schedule with their child.
At our house, we have a dry-erase calendar posted on the wall. Every Sunday evening, I write both of my children’s schedules for the following week–including homework time. We go through the calendar together, and they reference it often throughout the week. I can tell both my son and daughter feel better when they know when they’ll get their homework done.
2. Create a Homework Space
Ideally, your child should have a dedicated homework space. It doesn’t matter if that space is a desk, a dining room table, or a kitchen countertop. What does matter is that the homework area is tidy, because an unorganized homework area is very distracting.
3. Start Homework Early
Encourage your child to start their homework as early as possible. Help them review their assignments, make a plan for what needs to be completed, and then dive in. Naturally, children are more tired later in the evening which can lead to more stress.
4. Encourage Breaks
If you can see your child becoming frustrated or overwhelmed by their homework, encourage them to take a breather and come back to it later. As a teacher and tutor, I called this a “brain break” and believe these breaks are essential. Taking a short break will give your child a chance to step away from a frustrating problem or assignment.
5. It’s Okay to Ask for Help
Sometimes, homework can become just too stressful and overwhelming. In that case, it really is okay to stop. Children can learn to advocate for themselves by making a list of questions for their teacher and asking for help the next day. Depending on their age, you might need to help role-play how to approach their teacher with their frustrations.
Additionally, parents should never feel afraid to contact their child’s teacher to talk about homework issues. When I was teaching elementary school, I always wanted parents to feel comfortable reaching out about any issues, including homework stress.
6. Get Plenty of Rest
Sleep is critical to a child’s overall wellbeing , which includes their academic performance. Tired kids can’t concentrate as well, which can lead to feeling more overwhelmed about homework assignments. According to the American Academy of Sleep Medicine, kids aged 6-12 should get at least 9 hours of sleep each night.
7. Consider a Homework Group
Organizing a homework group a few times a week is another way for your child to view homework more positively. Working as a group encourages collaboration, while discussions can solidify concepts learned in class.
8. Encourage Positivity
No matter what your school experience was like, it’s important to model a growth mindset for your child. A growth mindset is the belief that your abilities can develop and improve over time. So if your child says something like “ I can’t do this! ” first acknowledge their frustration. Then, encourage them to say, “ I may not understand this yet, but I will figure it out. ” Speaking positively about tough experiences takes practice, but it will go a long way in reducing homework stress for your child.
9. Develop Skills With Fun Games
Feeling stressed about homework is no fun. Completing worksheets and memorizing facts is necessary, but playing games is a great way to inject some excitement into learning. Doodle’s interactive math app is filled with interactive exercises, engaging math games, and unique rewards that help kids develop their skills while having fun.
Lower Math Anxiety with DoodleMath
Does your child struggle with math anxiety? DoodleMath is an award-winning math app f illed with fun, interactive math questions aligned to state standards. Doodle creates a unique work program tailored to each child’s skill level to boost confidence and reduce math anxiety. Try it free today!

FAQs About Homework Stress
Many studies have shown that homework and stress often go hand-in-hand, often because many children feel pressure to perform perfectly or they have trouble managing their emotions–they get overwhelmed or flooded easily.
You can help your child reduce homework stress in several ways, including by establishing a routine, creating a homework space, encouraging breaks, and making homework fun with online games or math apps.

Lesson credits

Katie Wickliff
Katie holds a master’s degree in Education from the University of Colorado and a bachelor’s degree in both Journalism and English from The University of Iowa. She has over 15 years of education experience as a K-12 classroom teacher and Orton-Gillingham certified tutor. Most importantly, Katie is the mother of two elementary students, ages 8 and 11. She is passionate about math education and firmly believes that the right tools and support will help every student reach their full potential.
Parents, sign up for a DoodleMath subscription and see your child become a math wizard!

What we offer
Quick links
All rights reserved.

Are you a parent, teacher or student?
Get started for free!
Maths information pack
We ask for your contact info so we can send our info pack directly to your inbox for your convenience, exam prep information pack, case studies information pack.
Book a chat with our team

I’m new to Doodle

My school is already using Doodle

Information pack
We ask for your contact info so that our education consultants can get in touch with you and let you know a bit more about doodle., student login, which programme would you like to use.

DoodleMaths
DoodleTables
DoodleEnglish
DoodleSpell
If you’d like to use Doodle’s browser version, please visit this page on a desktop.
To log in to Doodle on this device, you can do so through our apps. You can find out how to download them here:
- How It Works
- Sleep Meditation
- VA Workers and Veterans

- How It Works 01
- Sleep Meditation 02
- Mental Fitness 03
- Neurofeedback 04
- Healium for Business 05
- VA Workers and Veterans 06
- Sports Meditation 07
- VR Experiences 08
- Social Purpose 11
Does Homework Cause Stress? Exploring the Impact on Students’ Mental Health
How much homework is too much?

Homework has become a matter of concern for educators, parents, and researchers due to its potential effects on students’ stress levels. It’s no secret students often find themselves grappling with high levels of stress and anxiety throughout their academic careers, so understanding the extent to which homework affects those stress levels is important.
By delving into the latest research and understanding the underlying factors at play, we hope to curate insights for educators, parents, and students who are wondering whether homework causing stress in their lives?
The Link Between Homework and Stress: What the Research Says
Over the years, numerous studies investigated the relationship between homework and stress levels in students.
One study published in the Journal of Experimental Education found that students who reported spending more than two hours per night on homework experienced higher stress levels and physical health issues . Those same students reported over three hours of homework a night on average.
This study, conducted by Stanford lecturer Denise Pope, has been heavily cited throughout the years, with WebMD producing the below video on the topic– part of their special report series on teens and stress :
Additional studies published by Sleep Health Journal found that long hours on homework on may be a risk factor for depression , suggesting that reducing workload outside of class may benefit sleep and mental fitness .
Homework’s Potential Impact on Mental Health and Well-being
Homework-induced stress on students can involve both psychological and physiological side effects.
1. Potential Psychological Effects of Homework-Induced Stress:
• Anxiety: The pressure to perform well academically and meet homework expectations can lead to heightened levels of anxiety in students. Constant worry about completing assignments on time and achieving high grades can be overwhelming.
• Sleep Disturbances : Homework-related stress can disrupt students’ sleep patterns, leading to sleep anxiety or sleep deprivation, both of which can negatively impact cognitive function and emotional regulation.
• Reduced Motivation: Excessive homework demands could drain students’ motivation, causing them to feel fatigued and disengaged from their studies. Reduced motivation may lead to a lack of interest in learning, hindering students’ overall academic performance.
2. Potential Physiological Effects of Homework-Induced Stress:
• Impaired Immune Function: Prolonged stress could weaken the immune system, making students more susceptible to illnesses and infections.
• Disrupted Hormonal Balance : The body’s stress response triggers the release of hormones like cortisol, which, when chronically elevated due to stress, can disrupt the delicate hormonal balance and lead to various health issues.
• Gastrointestinal Disturbances: Stress has been known to affect the gastrointestinal system, leading to symptoms such as stomachaches, nausea, and other digestive problems.
• Cardiovascular Impact: The increased heart rate and elevated blood pressure associated with stress can strain the cardiovascular system, potentially increasing the risk of heart-related issues in the long run.
• Brain impact: Prolonged exposure to stress hormones may impact the brain’s functioning , affecting memory, concentration, and other cognitive abilities.
The Benefits of Homework
It’s important to note that homework also offers many benefits that contribute to students’ academic growth and development, such as:
• Development of Time Management Skills: Completing homework within specified deadlines encourages students to manage their time efficiently. This valuable skill extends beyond academics and becomes essential in various aspects of life.
• Preparation for Future Challenges : Homework helps prepare students for future academic challenges and responsibilities. It fosters a sense of discipline and responsibility, qualities that are crucial for success in higher education and professional life.
• Enhanced Problem-Solving Abilities: Homework often presents students with challenging problems to solve. Tackling these problems independently nurtures critical thinking and problem-solving skills.
While homework can foster discipline, time management, and self-directed learning, the middle ground may be to strike a balance that promotes both academic growth and mental well-being .
How Much Homework Should Teachers Assign?
As a general guideline, educators suggest assigning a workload that allows students to grasp concepts effectively without overwhelming them . Quality over quantity is key, ensuring that homework assignments are purposeful, relevant, and targeted towards specific objectives.
Advice for Students: How to balance Homework and Well-being
Finding a balance between academic responsibilities and well-being is crucial for students. Here are some practical tips and techniques to help manage homework-related stress and foster a healthier approach to learning:
• Effective Time Management : Encourage students to create a structured study schedule that allocates sufficient time for homework, breaks, and other activities. Prioritizing tasks and setting realistic goals can prevent last-minute rushes and reduce the feeling of being overwhelmed.
• Break Tasks into Smaller Chunks : Large assignments can be daunting and may contribute to stress. Students should break such tasks into smaller, manageable parts. This approach not only makes the workload seem less intimidating but also provides a sense of accomplishment as each section is completed.
• Find a Distraction-Free Zone : Establish a designated study area that is free from distractions like smartphones, television, or social media. This setting will improve focus and productivity, reducing time needed to complete homework.
• Be Active : Regular exercise is known to reduce stress and enhance mood. Encourage students to incorporate physical activity into their daily routine, whether it’s going for a walk, playing a sport, or doing yoga.
• Practice Mindfulness and Relaxation Techniques : Encourage students to engage in mindfulness practices, such as deep breathing exercises or meditation, to alleviate stress and improve concentration. Taking short breaks to relax and clear the mind can enhance overall well-being and cognitive performance.
• Seek Support : Teachers, parents, and school counselors play an essential role in supporting students. Create an open and supportive environment where students feel comfortable expressing their concerns and seeking help when needed.
How Healium is Helping in Schools
Stress is caused by so many factors and not just the amount of work students are taking home. Our company created a virtual reality stress management solution… a mental fitness tool called “Healium” that’s teaching students how to learn to self-regulate their stress and downshift in a drugless way. Schools implementing Healium have seen improvements from supporting dysregulated students and ADHD challenges to empowering students with body awareness and learning to self-regulate stress . Here’s one of their stories.
By providing students with the tools they need to self-manage stress and anxiety, we represent a forward-looking approach to education that prioritizes the holistic development of every student.
To learn more about how Healium works, watch the video below.
About the Author

Sarah Hill , a former interactive TV news journalist at NBC, ABC, and CBS affiliates in Missouri, gained recognition for pioneering interactive news broadcasting using Google Hangouts. She is now the CEO of Healium, the world’s first biometrically powered immersive media channel, helping those with stress, anxiety, insomnia, and other struggles through biofeedback storytelling. With patents, clinical validation, and over seven million views, she has reshaped the landscape of immersive media.
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- HHS Author Manuscripts
The Role of Exercise in Management of Mental Health Disorders: An Integrative Review
Patrick j. smith.
1 Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham, North Carolina 27708, USA;
2 Department of Medicine, Duke University Medical Center, Durham, North Carolina 27708, USA;
3 Department of Population Health Sciences, Duke University Medical Center, Durham, North Carolina 27708, USA;
Rhonda M. Merwin
A large and growing body of evidence suggests that physical activity (PA) may hold therapeutic promise in the management of mental health disorders. Most evidence linking PA to mental health outcomes has focused on the effects of aerobic exercise training on depression, although a growing body of work supports the efficacy of both aerobic and resistance exercise paradigms in the treatment of anxiety and post-traumatic stress disorder. Despite abundant evidence linking PA and mental health, use of exercise training as a mental health treatment remains limited due to three important sources of uncertainty: ( a ) large individual differences in response to exercise treatment within multiple mental health domains; ( b ) the critical importance of sustained PA engagement, not always achieved, for therapeutic benefit; and ( c ) disagreement regarding the relative importance of putative therapeutic mechanisms. Our review of treatment data on exercise interventions and mental health outcomes focuses primarily on depression and anxiety within a health neuroscience framework. Within this conceptual framework, neurobiological and behavioral mechanisms may have additive or synergistic influences on key cognitive and behavioral processes that influence mental health outcomes. We therefore highlight sources of treatment heterogeneity by integrating the critical influences of ( a ) neurobiological mechanisms enhancing neuroplasticity and ( b ) behavioral learning of self-regulatory skills. Understanding the interrelationships between dynamic neurobiological and behavioral mechanisms may help inform personalized mental health treatments and clarify why, and for whom, exercise improves mental health outcomes. The review concludes with recommendations for future studies leveraging individual differences to refine treatment approaches to optimize mental health benefits.
EPIDEMIOLOGICAL EVIDENCE LINKING PHYSICAL ACTIVITY AND MENTAL HEALTH
Numerous epidemiological studies have demonstrated that lower amounts of physical activity (PA) or greater amounts of time spent in sedentary behaviors are associated with greater risk of poor mental health. In a recent study of 1.2 million US adults, in which participants were matched across numerous background and demographic factors, individuals who exercised reported better mental health functioning compared to nonexercisers ( 1 ). Prospective studies focusing on specific mental health conditions have reported similar findings, suggesting that greater habitual PA may protect against the development of various mental health conditions. For example, a recent meta-analysis of 49 prospective studies across nearly 267,000 individuals demonstrated that higher levels of PA associated with reduced odds of developing depression [odds ratio (OR) = 0.83, 95% confidence interval (CI) 0.79–0.88] across age groups ( 2 ). PA also prospectively associated with lower odds of developing elevated anxiety symptoms (OR = 0.87, 95% CI 0.77–0.99) and anxiety disorders (OR = 0.66, 95% CI 0.53–0.83) in a recent meta-analysis of more than 80,000 individuals ( 3 ).
The concept of habitual PA serving a protective role against the development of mental health conditions is further bolstered by data suggesting that greater amounts of PA are associated with incrementally lower risk of mental health problems. Across various exercise modalities, there appears to be a dose-response association between greater PA and mental health functioning ( 4 ), even after accounting for numerous social, medical, and behavioral confounds, such as smoking (OR = 0.67, 95% CI 0.61–0.75) ( 5 ). Individuals with moderate or low levels of fitness exhibit a 23% and 47% greater risk of developing a mental health problem when compared to their highly fit counterparts, with additive benefits of aerobic and resistance exercise ( 6 ). Taken together, epidemiological evidence provides robust evidence that greater habitual PA associates with better mental health functioning. For the purposes of the present review, exercise is defined as planned or intentional training activities, whereas PA also includes leisure-time activities.
Exercise Training and Mental Health: Experimental Evidence
Results from randomized trials of exercise, while generally favorable, have been more mixed than observational findings ( 7 – 10 ). Multiple meta-analytic studies have examined the impact of exercise training, primarily aerobic but also resistance training ( 10 ), with varying degrees of efficacy depending on methodological considerations, including study quality, duration ( 11 ), and choice of comparator group ( 12 ). Most evidence suggests that exercise, particularly aerobic training, improves depression- and anxiety-related outcomes compared with attention control conditions, with treatment effect sizes paralleling those for conventional pharmacotherapeutic approaches. Aerobic exercise trials have generally reported moderate to large improvements compared with no intervention [effect size (ES) = 1.24] or conventional control conditions (ES = 0.68), with improvements comparable to standard psychological or pharmacological approaches. Importantly, the effects of exercise training tend to decline over time and are generally not significant at follow-up (ES = 0.22) ( 8 ), with therapeutic benefits only sustained among individuals who continue to exercise following cessation of active treatment ( 13 ). Although fewer studies have examined resistance training paradigms, existing data suggest that resistance training also appears to improve depressive symptoms (ES = 0.66, 95% CI 0.48–0.83), albeit with significant heterogeneity across trials ( 10 ). Exercise training has also been examined as an add-on therapy, enhancing the efficacy of conventional outpatient treatment approaches over the course of 2–3 months (ES = −0.79, 95% CI −1.01 − −0.57) ( 7 ).
Interestingly, evidence for dose-response effects of training is less robust than observational findings; relatively few studies link the degree of improvement with the intensity or duration of training ( 14 ). In addition, examination of sustained treatment response over time suggests that the most important factor associating with remission from various mental health conditions is the degree of exercise maintenance over time, regardless of initial intervention assignment, with continued exercise participation demonstrating a threshold of benefit corresponding closely to the American Heart Association’s recommended level of activity of 150 min per week ( 13 , 15 ). In summary, exercise training appears to have a potentially important impact on mental health functioning, comparable to conventional psychotherapeutic and pharmacological approaches; however, the effects of exercise training vary across patient populations and training modalities, and the long-term mental health benefits appear contingent upon sustained PA engagement. Understanding the mechanisms of treatment response and exercise maintenance is therefore of critical importance to the ultimate efficacy of exercise as a clinical treatment.
Transdiagnostic Mechanisms
Recent studies have begun to examine transdiagnostic mechanisms by which exercise may improve mental health outcomes ( 16 ), including integration of interrelated behavioral and neurobehavioral domains ( 17 , 18 ). For example, recent literature syntheses have begun integrating affective and cognitive mechanisms of treatment across samples of patients with neurodegenerative disorders and depression, demonstrating that exercise improves depressive symptoms (ES = 0.78), with weak dose-response effects (standardized beta = 0.007, p = 0.012). Improvements in depression were paralleled by improvements in behavioral markers of cognitive control (ES = 0.24), with a high degree of heterogeneity ( 16 ). While methodological variation is frequently and appropriately identified as a source of heterogeneity, the impact of exercise on mental health outcomes also appears to vary based on the presence and type of neurobehavioral impairment.
An illustrative example of diagnostic treatment heterogeneity is the use of exercise among individuals with late-life depression (LLD) ( 19 , 20 ) and/or vascular depression ( 21 ). These individuals demonstrate substantially poorer treatment outcomes to conventional therapeutic approaches compared to younger individuals with depression or individuals with an earlier first depressive episode, despite ostensibly meeting the same diagnostic criteria. Individuals with LLD are more likely to have cardiovascular disease risk factors, white matter hyperintensities, and comorbid cognitive dysfunction typified by executive function impairments than individuals with an earlier onset of depression. Despite these patients’ lower treatment response, psychomotor activation appears to be an important protective factor, predicting subsequent persistence of treatment benefits ( 22 ). The effects of exercise training in this population have been heterogeneous; some large, multisite trials have failed to find a benefit of exercise in LLD samples ( 23 ). Nevertheless, in a recent meta-analysis of nine trials and 1,308 participants, exercise training was found to be moderately effective in reducing depressive symptoms (ES = 0.64, 95% CI 0.27–1.01), with significant heterogeneity across studies ( 9 ). Follow-up analyses suggested that greater age, cognitive impairment, and severity of depressive symptoms all contributed to treatment response heterogeneity, despite evidence for favorable exercise effects both among older adults ( 24 ) and in selected trials among individuals with dementia. These analyses suggested that the observed lack of treatment response in some individuals may be due to a greater prevalence of impairments in reward system pathways in individuals with geriatric depression or LLD. Existing evidence linking exercise training to mental health outcomes suggests that exercise has beneficial effects with wide variation, but there is a lack of explanatory studies delineating for whom and why exercise is beneficial.
EXERCISE TRAINING AND MENTAL HEALTH: EXPLANATORY MECHANISMS
Examination of the literature linking exercise to mental health suggests that exercise training is beneficial for a broad array of mental health outcomes, although the strength of treatment benefit appears to vary across populations and training modalities. The present literature base could be characterized as having three overarching mechanistic hypotheses, which are useful in framing hypotheses regarding treatment improvements: ( a ) Mental health is improved in association with physical/hedonic effects of exercise, ( b ) exercise improves mental health via neurobiological mechanisms, or ( c ) exercise is a vehicle for cultivating behavioral mechanisms of change (e.g., self-regulatory skills and self-efficacy). We contend that exercise training likely improves mental health through synergistic influences of both neurobiological and behavioral learning mechanisms ( Figure 1 ). Within this framework ( 25 , 26 ), training improves neurobiological systems critical for adaptive learning, as well as affective and cognitive control processes, resulting in synergistic improvements in the regulation of both cognitive and affective responses through a “virtuous circle” of reinforcement ( 27 , 28 ).

Conceptual model integrating neurobiological and behavioral mechanisms by which exercise training improves mental health outcomes.
Core Influence of Neuroplasticity
Neuroplasticity is increasingly characterized as a central mechanistic component of mental health improvements and is highly influenced by PA. The brain’s capacity for neurobiological remodeling within key neurocircuitry is a critical element of adaptive learning, is impaired across many heterogeneous mental health conditions, declines with age, and may be inhibited by several age-related systemic processes. Adaptive learning, in turn, is a critical element of mental health improvements following behavioral interventions. Increased neuroplastic capacity is one hypothesized mechanism underlying the mental health benefits of several widely used somatic psychiatric treatment modalities, including selective serotonin reuptake inhibitors and transmagnetic stimulation. Exercise is one of the few behavioral processes that appears to increase neuroplasticity.
At the structural level, neuroplasticity has been used to refer to the growth of new neurons and glial cells (neurogenesis), as well as new connections between existing neural networks through dendritic remodeling, synaptic formation and pruning, and axonal augmentation (synaptogenesis). Additional, related changes include the growth of new microvascular pathways (angiogenesis) and potentiation of neurotransmitter systems (monoamines) that are important for reward sensitization. There is now a general consensus that in adult humans, neurogenesis occurs in two specific brain regions, both of which are critical for mental health disorders and treatments: ( a ) the sub-granular zone of the dentate gyrus (mesial temporal lobe) and ( b ) the subventricular zone adjacent to the caudate and striatum (subcortex-prefrontal cortex). The dentate gyrus is essential for the creation and consolidation of new memories and regulation of affect, primarily changing through new gray matter cell growth. The subventricular zone and caudate are critical to striatal dopamine function and subcortical white matter pathways ( 29 ). Multiple lines of evidence suggest that neuroplastic changes and enhanced learning ability as a behavioral corollary are crucial therapeutic substrates for successful treatment outcomes ( Figure 2 ).

Conceptual model of neurobiological mechanisms by which exercise training improves mental health outcomes. Abbreviations: BDNF, brain-derived neurotrophic factor; IGF-1, insulin-like growth factor 1; VEGF, vascular endothelial growth factor.
Neuroplasticity Facilitators
Several key systemic factors must be present to facilitate neuroplastic changes, all of which are modifiable through exercise training. Briefly, these include neurotrophins, intact cerebral metabolic function, low neuroinflammation, and sleep. Neurotrophic growth factors are enhanced by exercise and linked to neuroplasticity, including modulation of brain-derived neurotrophic factor (BDNF), vascular endothelial growth factor (VEGF), and insulin-like growth factor 1 (IGF-1). BDNF is increased following aerobic ( 30 ) and resistance exercise training ( 31 ) and is critical to neurogenesis in the dentate gyrus. VEGF is more closely tied to cerebrovascular and microglial function, as well as angiogenesis. IGF-1 is more closely tied to cerebral and systemic metabolic changes, conferring structural adaptations similar to those seen with BDNF.
Neuroplasticity Inhibitors
Growth factors, particularly BDNF, also have systemic effects in regulating cellular bioenergetic function ( 32 ), which is disrupted in multiple mental health conditions ( 33 ), making it more difficult to facilitate affective control, cultivate flexible response patterns, or facilitate synaptic plasticity adaptations within supportive neurocircuitry ( 34 ). The bioenergetic system is also highly influenced by inflammation ( 35 ), sharing multiple molecular pathways with neurogenesis and depression ( 36 ). Elevated levels of inflammation appear to inhibit the effects of aerobic exercise on enhanced neurogenesis ( 37 ), partly through increasing kynurenine accumulation in the brain. Exercise may facilitate skeletal muscle clearance of kynurenine, suggesting that the comparable effects of exercise and selective serotonin reuptake inhibitors on mental health outcomes may be due to their parallel, neuroprotective effects through kynurenine pathways ( 38 ).
EXERCISE TRAINING: BRAIN NETWORK ALTERATIONS
For the purposes of understanding the effects of exercise on critical brain neurocircuitry, existing evidence can be grouped into three categories. Changes are observed in three functional neuroanatomical circuits characterized in the triple network model of large-scale brain networks ( 39 ). As shown in Table 1 , these changes occur in the salience network (SN), the executive control network (ECN), and the default mode network (DMN). Both depression and anxiety are associated with lower volume within DMN (hippocampus) and SN (amygdala and anterior cingulate cortex) brain structures ( 40 ). Individuals with depression also demonstrate reduced connectivity between the ECN and DMN, whereas individuals with anxiety demonstrate reduced connectivity between the ECN and SN. Improvements following psychiatric treatments with disparate mechanisms also correlate with connectivity alterations between these key networks. For example, treatment-related improvements following emotion regulation (ER)–focused psychotherapy ( 41 ) associate with alterations in connectivity between the SN and DMN, with both networks demonstrating increased connectivity to the ECN following successful treatment. A similar pattern of improvements has been demonstrated following pharmacological treatment of depression with aberrant SN and DMN connectivity improving with treatment, as well as differential improvements across symptom clusters (emotional and somatic), type of antidepressant (noradrenergic and serotonergic), and pattern of altered connectivity ( 42 ). These findings have been interpreted as demonstrating that enhancing connectivity with the ECN associates with behavioral improvements in cognitive control (for SN connectivity) and reductions in overly self-referential processing (for DMN connectivity).
Large-scale brain networks relevant to exercise training and mental health outcomes
| Salience network (SN) | Executive control network (ECN) | Default mode network (DMN) | |
|---|---|---|---|
| Anterior insula, pregenual ACC, amygdala, ventral striatum | Dorsolateral PFC, dorsal ACC, posterior parietal cortex | Posterior cingulate cortex, ventromedial PFC, angular gyrus | |
| Function: goal-directed behavioral engagement, reward sensitization, energization, conflict resolution, motivated learning, interoception Dysfunction: disinhibition, apathy, poor integration of aversive interoceptive cues | Function: cognitive control, working memory, set maintenance, task monitoring and updating, cognitive flexibility, vigilance, metacognition Dysfunction: dysexecutive function, perseveration, impaired planning and time management, inattention | Function: self-referential processing, episodic memory and autobiographical retrieval, semantic memory, internal representations, and value-based decision making Dysfunction: impaired social cognition, memory impairment, verbal agnosia | |
| Norepinephrine, dopamine | Dopamine, GABA | Serotonin, acetylcholine, glutamate | |
| Stroop Interference, Go-No Go/Flanker tasks, Iowa Gambling Task, Verbal Fluency | Trail Making Test, Wisconsin Card Sorting Test, Tower of Hanoi, Digit Span, Mental Arithmetic | Logical Memory Test, California Verbal Learning Test, Benton Visual Memory Test, Boston Naming Test | |
| Function: approach-oriented coping, task perseverance, empathy Dysfunction: anhedonia, rumination, impulsivity, avoidant behaviors | Function: cognitive flexibility, adaptation to feedback, flexible attention Dysfunction: inflexible behavioral responses, inattention | Function: regulated affect, social sensitivity, appropriate self-context Dysfunction: poor affect regulation, generalized/self-referential memory | |
| Critical for initial training engagement, self-regulatory skills acquisition, sensitivity to reinforcement cues, regulation of aversive physical cues | Critical for self-regulatory skills generalization, exercise maintenance, flexible response patterns, adapting self-reinforcement strategies, monitoring progress, contingency management | Critical for relapse prevention, consolidation of new skills, affective control to manage psychosocial stressors, use of self-referential knowledge for behavioral maintenance | |
| Disrupted in GAD, PTSD, OCD, BPD, addiction, anorexia, pain disorders, Parkinson’s, vascular dementia, ADHD, and MDD | Disrupted in most psychiatric conditions including MDD, bipolar, schizophrenia, frontotemporal and vascular dementia, ADHD, autism | Disrupted across multiple conditions including amnestic MCI, Alzheimer’s, MDD, social anxiety disorder, and epilepsy |
ACC, anterior cingulate cortex; ADHD, attention-deficit/hyperactivity disorder; BPD, borderline personality disorder; GABA, gamma-aminobutyric acid; GAD, generalized anxiety disorder; MCI, mild cognitive impairment; MDD, major depressive disorder; OCD, obsessive compulsive disorder; PFC, prefrontal cortex; PTSD, posttraumatic stress disorder.
Volumetric changes following exercise training have been most consistently observed in the prefrontal cortex (PFC), subcortex, and mesial temporal brain structures ( 43 ), with the most consistent changes in the dentate gyrus ( 44 , 45 ). The mesial temporal lobe (MTL) is particularly vulnerable to neurodegenerative disease processes, such as Alzheimer’s disease, although exercise appears to increase volume in this brain region across both middle-aged and older adult samples ( 46 ). Moderate-intensity training in older adults, for example, increases hippocampal volume with dose-response improvements from 6 to 12 months, offsetting normative neurodegenerative changes (1–2% annually), without volumetric increases in other brain regions ( 47 ). In one of the few exercise trials collecting neuroimaging data from participants with depression, depressive symptoms improved in parallel with increased MTL volume and improved verbal memory, despite a 30% dropout rate and lack of a significant treatment group benefit ( 48 ).
While most randomized controlled trials (RCTs) have focused on MTL brain areas, white matter changes have also been reported, particularly in PFC and parietal lobe areas critical for SN and ECN function ( 43 ). In a one-year training intervention, Voss and colleagues ( 49 ) demonstrated improvements in microstructural parameters of white matter integrity in the PFC, paralleling improvements in MTL brain regions. Similarly, during a 10- to 12-year follow-up examination of participants in the LOOK-AHEAD diabetes trial, the lifestyle intervention group demonstrated an impressive 28% lower white matter hyperintensity volume, compared to only a 9% lower ventricle volume ( 50 ). We recently reported parallel results in a pilot study of adults with depression, in which aerobic exercise stabilized white matter hyperintensity progression following a 16-week treatment ( 51 ). Notably, preliminary evidence suggests similar improvements following resistance training, with participants exhibiting improvements in PFC white matter volume and executive functioning ( 52 ).
The effects of exercise training on connectivity changes extend studies of structural markers by elucidating their functional significance to underlying behavioral changes. Extant connectivity studies suggest critical influences impacting SN and ECN neurocircuitry, independent of volumetric changes in DMN brain structures. Acute exercise, for example, has been shown to enhance efficiency within the DMN and improve functional modulation between networks, as indicated by enhanced ability of SN and ECN brain regions to selectively and adaptively inhibit DMN functioning ( 53 ), with parallel improvements in behavioral markers of cognitive control ( 54 ). Several RCTs have suggested that exercise training may enhance connectivity in clinically important neurocircuitry ( 54 – 56 ), and some suggest that markers of brain connectivity hold central importance as translational biomarkers ( 55 ). Previous randomized trials of exercise training suggest that it may improve ECN and DMN markers of connectivity, with corresponding behavioral improvements. Voss and colleagues, for example, found that a 12-month aerobic exercise program among older adults enhanced ECN and DMN connectivity, with corresponding improvements in executive function ( 57 ). The DMN, in particular, has been extensively studied for its responsivity to exercise training ( 58 ), as well as being widely implicated in the pathogenesis of depression ( 59 , 60 ), particularly LLD ( 59 , 60 ). In addition, a growing body of work suggests that greater baseline evidence of disrupted connectivity is predictive of subsequent behavioral improvements in markers of cognitive control ( 55 , 56 ). Similar findings have been reported for mood improvements ( 61 ), with altered connectivity in DMN and ECN associating with poorer treatment outcomes and greater cognitive dysfunction among adults with depression ( 62 ).
Observed changes in connectivity are also likely attributable to enhancements of neurotransmitter systems, particularly neuromodulatory pathways (dopamine, norepinephrine, and (serotonin).
This assertion is supported by large amounts of indirect evidence suggesting that neurobehavioral improvements following exercise are largest in executive functions ( 17 , 18 ), which are preferentially impacted by dopaminergic disruption. In addition, parallel cognitive improvements are observed across heterogeneous populations with dysfunctional dopaminergic/norepinephrine functioning, including Parkinson’s disease ( 63 ), attention-deficit/hyperactivity disorder ( 64 , 65 ), and bipolar disorder ( 66 ), with exercise-related increases in dopamine production ( 67 ). Modulation of the serotonin system is also widely hypothesized to play an important mechanistic role in the effects of acute exercise training on mood-related changes ( 68 ), with at least one prior trial demonstrating that higher intensity of aerobic training increased plasma 5-HT levels, which associated with improved response inhibition ( 69 ). Taken together, these data suggest that enhanced production and synthesis of monoamines is a critical component of improved affect regulation and cognitive control, both of which enhance self-regulation.
EXERCISE TRAINING: BEHAVIORAL MECHANISMS
In addition to direct modulation of cognitive and affective responses, exercise training may also facilitate learning of adaptive behavioral responses that improve mental health ( Figure 1 ), broadly formulated as self-regulatory capacities. While self-regulation is vast, it includes ER and cognitive control, which are transdiagnostic mechanisms of change. Consistent with the Science of Behavior Change initiative ( 70 ), these mechanisms should be evaluable and coherent at different levels of analysis (i.e., changes in behavioral mechanisms should correspond to neurobiological changes) and, by extension, could be mutually facilitative, such that changes in one affect the other. Although prior research has examined regulation of both emotion and affect, affect regulation has traditionally been defined as the modulation of emotions or emotional expression in the service of self-regulation. Affect regulation has also traditionally been more closely associated with executive functioning in comparison with ER.
There are few examples that integrate psychological and neurocognitive mechanisms in a single model. One possible exception is self-systems theory (SST) ( 71 – 73 ). According to SST, many psychological disorders result from cumulative or catastrophic failures of goal pursuits ( 72 ). SST has most widely been used in depression, where it is superior to conventional therapeutic approaches among depressed adults with self-regulatory deficits ( 71 ). However, a critical conceptual element of SST, which parallels mechanistic studies on PA and mental health, is its integration of both psychological function and neurobiological inefficiencies as contributing to potential self-regulatory failures within an individual. Differential impact of exercise on mental health could arise from either source or from a lack of effective synergy between the two. This concept may be critical in understanding for whom interventions work and under what conditions, and in tailoring treatments.
Specific behavioral mechanisms linking exercise interventions to mental health include self-regulatory skills specific to affect regulation ( 61 , 74 ) (e.g., tolerating and modulating arousal) and cognition ( 75 ) (e.g., exerting cognitive control over behavior, sustaining attention, and flexibly shifting attention and behavioral responses to match environmental demands) ( 76 ), which could influence mental health directly and through increased self-efficacy ( 77 ). Exercise may also potentiate reward salience through increased engagement in personally meaningful or rewarding activities and reward sensitization, or improved fitness (e.g., feeling more fit, improved body image). Behavioral mechanisms broadly correspond with neurological domains of changes, as summarized in Figure 3 .

Conceptual model of behavioral mechanisms by which exercise training improves mental health outcomes.
EMOTION REGULATION/EXPERIENTIAL AVOIDANCE
The impact of exercise on mood is one of the most widely studied mechanisms linking exercise to mental health, both through acutely enhancing mood and by improving ER during stressful life circumstances ( 78 ). Newer cognitive-behavioral therapies (CBTs), such as Acceptance and Commitment Therapy ( 77 ) and Dialectical Behavior Therapy, target difficulties in ER as a key mechanism of change ( 79 ). ER is a multidimensional construct that includes awareness and clarity of feelings, as well as acceptance of emotions and the ability to modulate emotional responses. A significant literature indicates that difficulties in ER are associated with mental health problems and that improvements in ER correspond with better mental health. A smaller literature demonstrates improvements in these processes prospectively predicting outcomes. Experiential avoidance and avoidant coping with unwanted thoughts and feelings (i.e., efforts to avoid or suppress thoughts/feelings) are particularly detrimental, contributing to the development and maintenance of anxiety disorders (including panic disorder), depression, substance abuse, and posttraumatic stress disorder (PTSD), among others. Related issues of hypervigilance, reactive or impulsive responding to internal cues, and difficulty labeling emotions (alexithymia or poor interoceptive awareness) are also implicated in psychiatric disorders, most notably PTSD, borderline personality disorder, and eating disorders.
Exercise may improve individuals’ ability to tolerate negative affect or high levels of arousal. For example, high-intensity exercise elicits autonomic arousal that mimics anxiety. During exercise, individuals experience these sensations in a nonthreatening context, in which aversive interoceptive cues are not only expected but may be indicative of effective engagement. This may form new associations with anxiety and increase capacity to tolerate interoceptive sensations while inhibiting avoidance/escape responses. Participants may also learn skills to modulate arousal, such as through paced breathing. Exercise training, particularly high intensity interval training and resistance training, also causes temporary discomfort in pursuit of a more long-term goal (e.g., fitness). The ability to allow short-term discomfort in favor of long-term gain is essential for impulse control. Repeated exercise training over the course of weeks and gradual intensity titration might be particularly effective in helping participants gain mastery over potentially distressing internal experiences. Exercise may therefore incorporate gradual exposure with response prevention in the context of training, similar to conventional psychotherapy paradigms using desensitization techniques through gradual exposure ( 80 – 82 ). Studies with various clinical populations have suggested that aerobic training reduces anxiety and anxiety sensitivity. Indeed, most of the brain regions that have enhanced activation and function following exercise training are well known for their importance in affective reactivity within the DMN pathways, particularly the ventromedial PFC and its regulation of reactivity within subcortical and insular brain regions ( 83 ). Decreased affect reactivity would be expected to decrease the need for unhealthy avoidance or suppression of emotional responses.
A separate line of research has examined changes in affective reactivity to provocative stimuli following exercise training in the setting of intentional weight loss. This work suggests that behavioral training exercise may diminish participant SN reactivity to salient food cues, particularly within the ventral striatum and insula ( 84 ). In a similar study using a crossover design ( 85 ), 60 min of exercise among habitual exercisers reduced activation in the putamen and peri-insular brain regions to high-energy food cues. Similarly, Cornier and colleagues ( 84 ) found that reductions in weight were associated with reduced insular activation among overweight/obese adults following a 6-month exercise trial. Taken together, this work suggests that exercise might decrease affective reactivity/saliency of food cues, increasing ability to control impulses or regulate eating behavior. Increased modulation of food responses may also have broader implications for cultivating impulse control and self-regulatory capacity, which holds importance for reduced substance use risk, behavioral impulsivity, and overall improvements in mental health functioning.
COGNITIVE CONTROL/FLEXIBILITY
Exercise training programs often include behavior change strategies in the context of intervention delivery, particularly for home-based training paradigms. Behavior change strategies include behavioral self-regulatory skills such as goal setting, activity planning (including behavioral activation), adaptive problem solving, the provision of feedback, and self-monitoring ( 86 ), all of which overlap with key elements of traditional CBT. When these strategies are utilized in behavioral trials among individuals with mental health conditions, they likely play an active therapeutic role and may partially explain treatment improvements ( 87 ). As detailed below, effective behavioral engagement and self-monitoring are frequently impaired in individuals with depression and anxiety. Interventions cultivating these skill sets may therefore offer opportunities for experiential practice of clinically relevant skill domains in the service of exercise titration and maintenance.
Conventional exercise training programs teach participants to identify and implement goals that are specific, measurable, achievable, realistic, and timely (SMART goals), in order to optimize exercise participation and maintenance. Through the process of setting SMART goals, striving toward them, and evaluating iterative progress, participants cultivate realistic expectations for themselves and internalize a sense of behavioral control. Realistic goal setting and attainment also contribute to ER by increasing self-mastery, increasing agency, and establishing new, positive associations with self-concept. The process of self-monitoring (tracking behavior and its consequences) may also build a greater capacity to identify and repeat behaviors that are effective, as well as identifying maladaptive behavioral patterns.
Several mental health conditions, including depression and anxiety, are notable for impairments in cognitive flexibility and attentional control. Difficulties include poor set-shifting abilities (i.e., difficulty switching between tasks or altering behavior in response to feedback) ( 88 ), selective attention, and distractibility. Sustained attention and vigilance are also impaired across many mental health conditions, particularly in depression, where patients have difficulties sustaining engagement toward goal-directed targets over prolonged periods of time. Competing cognitive processes, such as rumination or excessive worry, may divert attention away from effective task performance and increase emotional suffering.
Impairments in cognitive control domains, including cognitive flexibility and executive function, have been repeatedly tied to behavioral treatment outcomes ( 89 – 91 ). Similarly, behavioral treatments improving cognitive flexibility and executive function also tend to favorably impact depression and anxiety outcomes ( 89 ). For example, cognitive flexibility is a putative treatment mechanism of mindfulness-based stress reduction, which has been shown to increase resting-state connectivity within ECN brain areas following training ( 92 ). As noted above, exercise training appears to have preferentially favorable effects on executive functions ( 76 ) and connectivity within ECN brain areas ( 57 ). Notably, poorer cognitive control is also a robust predictor of inadequate PA maintenance ( 28 , 93 ), suggesting that poorer cognitive control is likely to present barriers both for initial acquisition of self-regulatory skills for PA engagement and utilization of these skills for maintenance over time.
Several newer CBTs teach mindfulness to decrease engagement in unproductive mental activities and improve capacity to be in the present moment. Exercise training programs may increase the ability to direct and sustain attention to the present, particularly if exercises are sufficiently difficult. In this case, effective engagement in the activity requires full attention to the task and awareness of a narrowed set of stimuli (e.g., one’s breathing and ability to pace breathing). These behavioral mechanisms may change in tandem with neurobiological-mediated decreases in the saliency of some stimuli (described above) and potentiation of reward, as detailed below.
Self-efficacy
Individual self-regulatory behaviors are also important for mental health functioning through their overlapping influences on self-efficacy ( 73 ). Broadly defined, self-efficacy refers to an individual’s confidence in their ability to achieve specific, personally significant goals. Greater engagement in PA has been shown to increase exercise self-efficacy ( 73 ), associated with improved body image and physical quality of life, and increases the likelihood of sustained PA maintenance over time ( 94 ). In addition, many of the domains reviewed above align closely with key conceptual elements of improved self-efficacy, including monitoring of performance accomplishments, behavioral modeling, social persuasion, and adaptive interpretation of physiological states. Recent meta-analytic syntheses suggest that exercise interventions confer moderately large improvements in self-efficacy across adolescent and adult cohorts (ES = 0.59) ( 95 ). The total number of behavior change strategies demonstrates the strongest associations with improved PA, regardless of the specific strategy used ( 96 ).
Reinforcement/Reward
A poverty of reinforcement or adaptive reward may lead to increased negative affect (e.g., depression) or the development of maladaptive behavior patterns to increase positive feelings (e.g., substance abuse). There is an extensive literature on increasing reinforcers/reward as a treatment mechanism of depression through behavioral activation ( 97 ). Newer CBTs, such as Acceptance and Commitment Therapy, link behavioral activation specifically to personal values, which may function to augment its reinforcement value or function as an establishing operation, and/or help sustain activity engagement. Behavioral activation often includes exercise or other forms of PA and may therefore both increase opportunities for positive reinforcement and cultivate realistic expectations regarding loss and reward, both of which may improve mental health. In addition, individual differences in reward sensitivity likely explain part of the observed heterogeneity in intermediate, positive consequences of PA (e.g., improved mood or fitness), which have been associated with the self-reinforcing nature of habitual PA and maintenance ( 74 ).
Dysfunctional reward sensitivity is a core feature increasing the risk of depression and serves as a key barrier to implementation of many therapeutic interventions. Exercise training has been postulated to improve reward sensitivity by augmenting dopaminergic function. Focusing on goal-directed behaviors has been shown to enhance top-down activation within the ventromedial PFC and ventral striatum, as well as downregulating insular and amygdala activation during stressful activities ( 98 ). Individuals engaging in habitual PA demonstrate differential activation of the ventral striatum, a critical dopamine hub, compared to their sedentary counterparts following acute exercise training ( 99 ). Individuals accustomed to habitual PA also show improved reward system functioning compared to sedentary counterparts, a relationship that does not appear to differ based on physical fitness ( 100 ).
FUTURE DIRECTIONS FOR TAILORED TREATMENTS
Clearly specifying both neurological and behavioral mechanisms that link exercise to mental health and how they might interact synergistically to produce outcomes may have implications for the design of exercise programs to potentiate training engagement and optimize outcomes for individuals or groups of individuals. Pre-existing neurobiological differences might explain the extent to which exercise interventions are effectively engaged and/or suggest indirect mechanisms of benefit in the context of exercise training. Repeated measurement and network analyses may be able to help disentangle the associations among elements that are probably mutually facilitative.
As reviewed above, both neurobiological markers of neuroplasticity and behavioral markers of self-regulatory function hold relevance in the development of future exercise training paradigms. Future studies should integrate phenotypic markers of neuroplasticity into intervention development in order to optimize intervention engagement. For example, individuals with blunted reward sensitivity may have difficulty with initial exercise engagement and therefore be less likely to adequately engage with or complete supervised training programs. These individuals may benefit from more gradual titration of activity, motivational priming prior to training sessions, or enhancement of reward reinforcement cues using external sources. Similarly, individuals with evidence of cognitive inflexibility and/or executive dysfunction may have difficulty with exercise maintenance and could benefit from receiving either greater external regulatory support (e.g., structured classes or exercise with a spouse) or additional self-management training to increase the likelihood of continued PA for optimal ER.
Future studies should also systematically assess and quantify individual differences in self-regulatory skills across participants, both as a baseline predictor of treatment engagement and across time as a mechanism of treatment improvements. Specifying individual differences in self-regulatory skills at baseline might also allow for effective treatment matching (matching individuals to exercise programs that they are more likely to be successful with or to programs that are more likely to address skill deficits and improve overall health and well-being) or tailoring of existing interventions to optimize outcomes. For example, individuals with difficulty regulating affect may also tend to avoid emotional or interoceptive discomfort, and they may experience increased sensitivity to arousal due to either distressing past experiences or inaccurate beliefs that arousal is dangerous. Irrespective of its precise origin, this behavioral tendency would suggest the need for differential titration of activity, greater usage of distraction techniques, or self-monitoring for titration based on external biometric sources (e.g., heart rate) that are not overly dependent on self-referential attention to interoceptive cues. These participants could also be trained to gain mastery by resisting urges to avoid or escape aversive cues or to use strategies to modulate arousal such that it can be sustained during a window of tolerance, which may be gradually expanded over time.
In addition, future RCTs may benefit from the use of optimization designs to determine the relative importance of priming neuroplasticity in order to achieve better mental health outcomes. RCTs utilizing sequential randomization to treat depression, for example, could re-randomize participants contingent upon connectivity or executive functioning changes, suggesting enhanced neuroplasticity as an intermediate marker of treatment responsivity. Similarly, trials examining exercise maintenance could benefit from provision of external support strategies among individuals with poorer self-regulatory capacity, including integration of social support or greater ease of access to exercise training equipment. Because these individuals will be less likely to self-initiate behavioral modifications or flexibly adapt their behavioral responses for exercise maintenance, additional environmental support is critical for outcomes.
CONCLUSIONS
In conclusion, aerobic and resistance exercise training hold promise in the treatment and management of mental health conditions, particularly depression and anxiety. Emerging evidence suggests that changes in underlying neuroplasticity may be an important individual difference explaining heterogeneous treatment benefits. In addition, underlying individual differences in neuroplasticity, either at baseline or in intervention-related changes, likely have significant implications for individuals developing and sustaining behavioral self-regulatory skills essential for mental health. These factors likely work in synergy, creating a “virtuous cycle” to predict long-term effects of exercise on mental health. By clearly specifying both neurobiological and behavioral mechanisms linking exercise to improved mental health, it may be possible to optimize treatment effects and personalize training approaches for maximal benefit.
LLD: late-life depression
SN: salience network
ECN: executive control network
DMN: default mode network
ER: emotion regulation
ACKNOWLEDGMENTS
Dr. Smith thanks Erica Shirts, Jeanne Schwartz, Bryan Feger, and Timothy Strauman for their thoughtful input during the conceptual formulation of this manuscript. This research was supported by funding from the National Institute of Health, NHLBI Grant R01HL130237.
DISCLOSURE STATEMENT
The authors are not aware of any affiliations, memberships, funding, or financial holdings that might be perceived as affecting the objectivity of this review.
LITERATURE CITED
COMMENTS
Pope and her colleagues found that too much homework can diminish its effectiveness and even be counterproductive. They cite prior research indicating that homework benefits plateau at about two hours per night, and that 90 minutes to two and a half hours is optimal for high school. • Greater stress: 56 percent of the students considered ...
Yes, and the stories we hear of kids being stressed out from too much homework—four or five hours of homework a night—are real. That's problematic for physical and mental health and overall well-being. But the research shows that higher-income students get a lot more homework than lower-income kids.
Despite the known benefits of regular physical activity, research shows a significant decline in physical activity participation and an increase in sedentary behavior during young adulthood during the college years. Studies examining the relationship ...
Homework improves brain function and enhances cognitive abilities. By practicing and repeating new skills through homework, students can enhance their memory and retain knowledge. Homework helps students build suitable study habits, learn time management, and realize personal responsibility. Homework fosters independence and the ability to use ...
Light-intensity exercise will elicit low but noticeable levels of physiological arousal, she said, which, in turn, presumably help to prime the brain for the intake of new information and the encoding of that information into memories. If the exercise is more vigorous, however, it may overstimulate the body and brain, she said, monopolizing ...
Homework has long been a source of debate, with parents, educators, and education specialists debating the advantages of at-home study. There are many pros and cons of homework. We've examined a few significant points to provide you with a summary of the benefits and disadvantages of homework.
Homework has its pros and cons, especially for college students. It can enhance critical thinking, time management, and learning, but it also brings stress, impacts mental health, and can become overwhelming. Finding the right balance is key. Focus on quality assignments, maintain flexibility, and make sure your homework complements rather than ...
Homework does not help younger students, and may not help high school students. We've known for a while that homework does not help elementary students. A 2006 study found that "homework had no association with achievement gains" when measured by standardized tests results or grades. [7]
Background: This study examined the effect of using physical activity homework on physical activity levels of college students. Methods: Students in randomly assigned sections of a university health course were assigned 30 minutes of physical activity homework 3 days a week or no homework for 12 weeks. Participants completed self-reports of ...
Homework can affect both students' physical and mental health. According to a study by Stanford University, 56 per cent of students considered homework a primary source of stress. Too much homework can result in lack of sleep, headaches, exhaustion and weight loss. Excessive homework can also result in poor eating habits, with families ...
Is Too Much Homework Bad for Kids' Health? Research shows that some students regularly receive higher amounts of homework than experts recommend, which may cause stress and negative health effects.
By creating a homework culture that emphasizes quality, provides timely feedback, and considers student circumstances, educators can optimize the positive impact of homework on student learning ...
A Stanford researcher found that students in high-achieving communities who spend too much time on homework experience more stress, physical health problems, a lack of balance and even alienation ...
The main barriers identified in high school and university students were lack of time, lack of motivation, and lack of accessible places. These findings may be useful in designing and implementing evidence-informed interventions and programs for physical activity promotion in students. 1.
After two hours, however, achievement doesn't improve. For high schoolers, Cooper's research suggests that two hours per night is optimal. If teens have more than two hours of homework a night, their academic success flatlines. But less is not better. The average high school student doing homework outperformed 69 percent of the students in ...
It's no secret that kids hate homework. And as students grapple with an ongoing pandemic that has had a wide-range of mental health impacts, is it time schools start listening to their pleas over ...
Chinese students spend more time on homework and other academic‐related work outside school hours and less time on screen viewing and sleep, compared to students of the same age from Western countries. However, less is known about the differences in physical activity and diet between Chinese and Western students.
Homework or Personal Lives? Many students get home and the first thing they do is homework. They're pressured by their parents to do their homework while simultaneously being encouraged to spend time with family, eat, spend time with friends, go outside, participate in sports or other extracurricular activities, and sleep for 7+ hours. Rather ...
What is homework anxiety? Find out why some kids get so anxious about homework, and how you can help.
Does it stress you out, numb your brain from busywork or actually make you fall behind in your classes? Should we get rid of homework? In " The Movement to End Homework Is Wrong, " published ...
Does homework cause stress? Effective strategies to reduce homework stress in elementary students from a private tutor & mom of two.
Uncover the effects of homework-induced stress on students' mental well-being and how to foster a balanced approach to education.
A large and growing body of evidence suggests that physical activity (PA) may hold therapeutic promise in the management of mental health disorders. Most evidence linking PA to mental health outcomes has focused on the effects of aerobic exercise training ...
Sticking to an exercise routine can also be difficult. For example, many people get bored doing the same exercises every day. To keep things fun and interesting, Tracy recommends switching up your activities. "It doesn't have to be running. It can be brisk walking. It can be hiking, cycling or using the elliptical" Tracy says.